
Abstract
Background
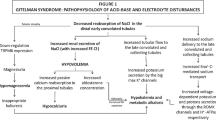
Patients with Gitelman syndrome, a hereditary salt-wasting tubulopathy, have loss-of-function mutations in the SLC12A3 gene coding for the thiazide-sensitive sodium chloride co-transporter in the distal convoluted tubule. Since the bulk of filtered phosphate is reabsorbed in the proximal tubule, renal phosphate wasting is considered exceptional in Gitelman syndrome.
Methods
We investigated the renal handling of inorganic phosphate in 12 unselected Italian patients affected with Gitelman syndrome (5 females and 7 males, aged 6.0–18 years, median age 12 years) and in 12 healthy subjects matched for gender and age (controls). The diagnosis of Gitelman syndrome among the patients had been made clinically and confirmed by molecular biology studies.
Results
The biochemical hallmarks of Gitelman syndrome, namely hypochloremia, hypokalemia, hypomagnesemia, increased urinary excretion of sodium, chloride, potassium and magnesium and reduced urinary excretion of calcium, were present in the 12 patients. In addition, both the plasma inorganic phosphate concentration (median and interquartile range: 1.28 [1.12–1.36] vs. 1.61 [1.51–1.66)] mmol/L) and the maximal tubular reabsorption of inorganic phosphate (1.08 [0.99–1.22] vs. 1.41 [1.38–1.47] mmol/L) were significantly lower (P < 0.001) in Gitelman patients than in control subjects. Circulating levels of 25-hydroxyvitamin D, intact parathyroid hormone and osteocalcin were similar in patients and controls.
Conclusions
The results of our case–control study disclose a hitherto unrecognized tendency towards renal phosphate wasting with mild to moderate hypophosphatemia in Gitelman syndrome.


Similar content being viewed by others


References
Dennis VW, Stead WW, Myers JL (1979) Renal handling of phosphate and calcium. Annu Rev Physiol 41:257–271
Knochel JP (1981) Hypophosphatemia. West J Med 134:15–26
Brame LA, White KE, Econs MJ (2004) Renal phosphate wasting disorders: clinical features and pathogenesis. Semin Nephrol 24:39–47
Proesmans W (2006) Threading through the mizmaze of Bartter syndrome. Pediatr Nephrol 21:896–902
Seyberth HW, Schlingmann KP (2011) Bartter- and Gitelman-like syndromes: salt-losing tubulopathies with loop or DCT defects. Pediatr Nephrol 26:1789–1802
Katopodis K, Elisaf M, Siamopoulos KC (1996) Hypophosphataemia in a patient with Gitelman’s syndrome. Nephrol Dial Transplant 11:2090–2092
Akhtar N, Hafeez F (2009) A rare case of Gitelman’s syndrome with hypophosphatemia. J Coll Physicians Surg Pak 19:257–259
Mastroianni N, Bettinelli A, Bianchetti M, Colussi G, De Fusco M, Sereni F, Ballabio A, Casari G (1996) Novel molecular variants of the Na-Cl cotransporter gene are responsible for Gitelman syndrome. Am J Hum Genet 59:1019–1026
Cruz DN, Shaer AJ, Bia MJ, Lifton RP, Simon DB, Yale Gitelman’s and Bartter’s Syndrome Collaborative Study Group (2001) Gitelman’s syndrome revisited: an evaluation of symptoms and health-related quality of life. Kidney Int 59:710–717
Syrén ML, Tedeschi S, Cesareo L, Bellantuono R, Colussi G, Procaccio M, Alì A, Domenici R, Malberti F, Sprocati M, Sacco M, Miglietti N, Edefonti A, Sereni F, Casari G, Coviello DA, Bettinelli A (2002) Identification of fifteen novel mutations in the SLC12A3 gene encoding the Na-Cl Co-transporter in Italian patients with Gitelman syndrome. Hum Mutat 20:78
Colussi G, Bettinelli A, Tedeschi S, De Ferrari ME, Syrén ML, Borsa N, Mattiello C, Casari G, Bianchetti MG (2007) A thiazide test for the diagnosis of renal tubular hypokalemic disorders. Clin J Am Soc Nephrol 2:454–460
von der Weid NX, Erni BM, Mamie C, Wagner HP, Bianchetti MG (1999) Cisplatin therapy in childhood: renal follow up 3 years or more after treatment. Nephrol Dial Transplant 14:1441–1444
Schwartz GJ, Work DF (2009) Measurement and estimation of GFR in children and adolescents. Clin J Am Soc Nephrol 4:1832–1843
Kruse K, Kracht U, Göpfert G (1982) Renal threshold phosphate concentration (TmPO4/GFR). Arch Dis Child 57:217–223
Burritt MF, Slockbower JM, Forsman RW, Offord KP, Bergstralh EJ, Smithson WA (1990) Pediatric reference intervals for 19 biologic variables in healthy children. Mayo Clin Proc 65:329–336
Velázquez H (1987) Thiazide diuretics. Ren Physiol 10:184–197
Antes LM, Fernandez PC (1998) Principles of diuretic therapy. Dis Mon 44:254–268
Puschett JB, Winaver J, Teredesai P (1980) Mechanism of the phosphaturia due to chlorothiazide. Adv Exp Med Biol 128:155–157
Peters N, Bettinelli A, Spicher I, Basilico E, Metta MG, Bianchetti MG (1995) Renal tubular function in children and adolescents with Gitelman’s syndrome, the hypocalciuric variant of Bartter’s syndrome. Nephrol Dial Transplant 10:1313–1319
de Muinich Keizer SM, Mul D (2001) Trends in pubertal development in Europe. Hum Reprod Updat 7:287–291
Gattineni J, Baum M (2012) Genetic disorders of phosphate regulation. Pediatr Nephrol 27:1477–1487
Wesseling-Perry K (2010) FGF-23 in bone biology. Pediatr Nephrol 25:603–608
Alon US (2011) Clinical practice. Fibroblast growth factor (FGF) 23: a new hormone. Eur J Pediatr 170:545–554
Lüthy C, Bettinelli A, Iselin S, Metta MG, Basilico E, Oetliker OH, Bianchetti MG (1995) Normal prostaglandinuria E2 in Gitelman’s syndrome, the hypocalciuric variant of Bartter’s syndrome. Am J Kidney Dis 25:824–828
Conflict of interest
None declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Viganò, C., Amoruso, C., Barretta, F. et al. Renal phosphate handling in Gitelman syndrome—the results of a case–control study. Pediatr Nephrol 28, 65–70 (2013). https://doi.org/10.1007/s00467-012-2297-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-012-2297-3