
Abstract
The aim of this retrospective cohort study was to describe the characteristics of patients with primary vesico-ureteral reflux (VUR) with special attention to gender-specific differences. Between 1970 and 2004, 735 patients were diagnosed with VUR and were systematically followed in a single tertiary renal unit. The following variables were analyzed: race, age at diagnosis, clinical presentation, weight and height Z-score, unilateral/bilateral reflux, VUR grade, renal damage, severity of renal damage, constipation, and dysfunctional voiding. Comparison of proportion between genders was assessed by the chi-square test with Yates’ correction. The logistic regression model was applied to identify independent variables associated with gender. A survival analysis was performed to evaluate VUR resolution. After adjustment, five variables remained independently associated with male gender at baseline: non-white race [Odds ratio (OR) = 1.98, 95% confidence interval (95% CI) 1.33–2.95, P=0.001], moderate/severe grade of reflux (OR=2.16, 95% CI 1.45–3.22, P<0.001), severe renal damage (OR=1.60, 95% CI 1.04–2.52, P=0.04), age at diagnosis <24 months (OR=1.79, 95% CI 1.23–2.60, P=0.002), and antenatal clinical presentation (OR=3.56, 95% CI 1.91–6.63, P<0.001). Follow-up data were available for 684 patients (93%). Median follow-up time was 69 months (range 6 months to 411 months). Girls had a greater risk of urinary tract infection (UTI) during follow-up than boys (OR=1.68, 95% CI 1.18–2.38, P=0.003). There was no difference in progression to chronic renal insufficiency (CRI) between boys (3.8%) and girls (2.4%) during this period of follow-up (OR=1.58, 95% CI 0.59–4.15, P=0.44). Gender as an isolated variable is a poor predictor of clinical outcome in an unselected series of primary reflux. Although boys had a more severe pattern at baseline, girls had a greater risk of dysfunctional voiding and recurrent UTI during follow-up.

Similar content being viewed by others


References
Fanos V, Cataldi L (2004) Antibiotics or surgery for vesicoureteric reflux in children. Lancet 364:1720–1722
Anderson PA, Rickwood AM (1991) Features of primary vesicoureteric reflux detected by prenatal sonography. Br J Urol 67:267–271
Burge DM, Griffiths MD, Malone PS, Atwell JD (1992) Fetal vesicoureteral reflux: outcome following conservative postnatal management. J Urol 148:1743–1745
Scott JE (1993) Fetal ureteric reflux: a follow-up study. Br J Urol 71:481–483
Yeung CK, Godley ML, Dhillon HK, Gordon I, Duffy PG, Ransley PG (1997) The characteristics of primary vesico-ureteric reflux in male and female infants with pre-natal hydronephrosis. Br J Urol 80: 319–327
Rolleston GL, Shannon FT, Utley WL (1970) Relationship of infantile vesicoureteric reflux to renal damage. BMJ 1:460–463
Smellie J, Edwards D, Hunter N, Normand IC, Prescod N (1975) Vesico-ureteric reflux and renal scarring. Kidney Int Suppl 4:S65–S72
Goldraich NP, Goldraich IH (1992) Followup of conservatively treated children with high and low grade vesicoureteral reflux: a prospective study. J Urol 148:1688–1692
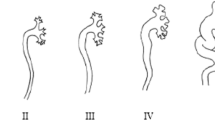
Lebowitz RL, Olbing H, Parkkulainen KV, Smellie JM, Tamminen-Mobius TE (1985) International system of radiographic grading of vesicoureteric reflux. International Reflux Study in Children. Pediatr Radiol 15:105–109
Silva JM, Diniz JS, Oliveira EA, Cardoso LS, Marino VS, Pimenta MR, Matos CC, Vieira SB (2003) Features of primary vesicoureteral reflux and renal damage in children at a single institution in Brazil from 1969 to 1999. Int Urol Nephrol 35:161–168
Schwartz GJ, Brion LP, Spitzer A (1987) The use of plasma creatinine concentration for estimating glomerular filtration rate in infants, children, and adolescents. Pediatr Clin North Am 34:571–590
(1987) Report of the Second Task Force on Blood Pressure Control in Children -1987. Task Force on Blood Pressure Control in Children. National Heart, Lung, and Blood Institute, Bethesda, Maryland. Pediatrics 79:1–25
(1996) Update on the 1987 Task Force Report on high blood pressure in children and adolescents. A working group report from the National High Blood Pressure Education Program. National High Blood Pressure Education Program Working Group on Hypertension Control in Children and Adolescents. Pediatrics 98:649–657
Filgueiras MF, Lima EM, Sanchez TM, Goulart EM, Menezes AC, Pires CR (2003) Bladder dysfunction: diagnosis with dynamic US. Radiology 227:340–344
Kaplan EL, Meier P (1958) Nonparametric estimation from incomplete observation. J Am Stat Assoc 53:457–481
Risdon RA (1993) The small scarred kidney in childhood. Pediatr Nephrol 7:361–364
Najmaldin A, Burge DM, Atwell JD (1990) Reflux nephropathy secondary to intrauterine vesicoureteric reflux. J Pediatr Surg 25:387–390
Oliveira EA, Diniz JS, Silva JM, Rabelo EA, Pontes AK, Souza MF (1998) Features of primary vesicoureteric reflux detected by investigation of fetal hydronephrosis. Int Urol Nephrol 30:535–541
Nguyen HT, Bauer SB, Peters CA, Connolly LP, Gobet R, Borer JG, Barnewolt CE, Ephraim PL, Treves ST, Retik AB (2000) 99m Technetium dimercapto-succinic acid renal scintigraphy abnormalities in infants with sterile high grade vesicoureteral reflux. J Urol 164:1674–1678
Lama G, Russo M, De Rosa E, Mansi L, Piscitelli A, Luongo I, Esposito Salsano M (2000) Primary vesicoureteric reflux and renal damage in the first year of life. Pediatr Nephrol 15:205–210
Nakai H, Kakizaki H, Konda R, Hayashi Y, Hosokawa S, Kawaguchi S, Matsuoka H, Nonomura K, Shimada K, Kawamura T (2003) Clinical characteristics of primary vesicoureteral reflux in infants: multicenter retrospective study in Japan. J Urol 169:309–312
Smellie JM, Prescod NP, Shaw PJ, Risdon RA, Bryant TN (1998) Childhood reflux and urinary infection: a follow-up of 10–41 years in 226 adults. Pediatr Nephrol 12:727–736
Marra G, Oppezzo C, Ardissino G, Dacco V, Testa S, Avolio L, Taioli E, Sereni F, ItalKid Project (2004) Severe vesicoureteral reflux and chronic renal failure: a condition peculiar to male gender? Data from the ItalKid Project. J Pediatr 144:677–681
Craig JC, Irwig LM, Knight JF, Roy LP (2000) Does treatment of vesicoureteric reflux in childhood prevent end-stage renal disease attributable to reflux nephropathy? Pediatrics 105:1236–1241
Koff SA, Wagner TT, Jayanthi VR (1998) The relationship among dysfunctional elimination syndromes, primary vesicoureteral reflux and urinary tract infections in children. J Urol 160:1019–1022
Chen JJ, Mao W, Homayoon K, Steinhardt GF (2004) A multivariate analysis of dysfunctional elimination syndrome, and its relationships with gender, urinary tract infection and vesicoureteral reflux in children. J Urol 171:1907–1910
Jodal U, Koskimies O, Hanson E, Lohr G, Olbing H, Smellie J, Tamminen-Mobius T (1992) Infection pattern in children with vesicoureteral reflux randomly allocated to operation or long-term antibacterial prophylaxis. The International Reflux Study in Children. J Urol 148:1650–1652
Sjostrom S, Sillen U, Bachelard M, Hansson S, Stokland E (2004) Spontaneous resolution of high grade infantile vesicoureteral reflux. J Urol 172:694–698
Verrier Jones K (1996) Vesico-ureteric reflux: a medical perspective on management. Pediatr Nephrol 10:795–797
Acknowledgments
This study was partially supported by CNPq (Brazilian National Research Council), Pró-Reitoria de Pesquisa (UFMG), and FAPEMIG. R.M.V. and M.A.V. were recipients of CNPq fellowships.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Silva, J.M.P., Oliveira, E.A., Diniz, J.S.S. et al. Gender and vesico-ureteral reflux: a multivariate analysis. Pediatr Nephrol 21, 510–516 (2006). https://doi.org/10.1007/s00467-006-0011-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-006-0011-z