
Abstract
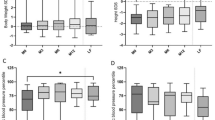
This study reports the benefits and side effects of conventional treatment, phosphate and calcitriol supplementation in patients with heritable hypophosphatemic rickets and a long-term follow-up, median of 60.9 months. The group is composed of 17 patients (ten girls). Sixteen patients presented with bone pain and/or deformities, and in one patient the diagnosis was radiological. All the patients had increased alkaline phosphatase, hypophosphatemia, decreased fractional phosphate tubular reabsorption (TRP) and maximum tubular phosphate reabsorption/glomerular filtration rate ratio (TPO4/GFR). Ten of 17 patients had metabolic acidosis, which was corrected only with the conventional treatment. Potassium citrate was prescribed to the patients who developed hypercalciuria. Excluding one patient with pulmonary dysfunction, the remaining 16 patients were divided into two groups according to the age at treatment onset (T0): group I (GI) ≥4 years (n =9) and GII <4 years (n =7). GI and GII had similar follow-up periods and treatment protocols. Seven out of nine GI patients underwent orthopedic surgery, in contrast to none of GII. Anthropometric data results showed that within each group there is no difference in weight and stature z -score at T0 and at the end of the observation (Tf), but, when both groups are compared, GII shows higher z -score for stature at T0 (p <0.05) and at Tf (p <0.05). Nephrocalcinosis developed in three cases and correlated with hypercalciuria (p <0.001) and dose of calcitriol (p =0.03). In conclusion, higher stature z -score is associated with early treatment. A careful protocol is recommended to detect such complications as nephrocalcinosis. We suggest potassium citrate for patients with hypercalciuria to avoid calcium precipitation.
Similar content being viewed by others


References
Tenehouse HS, Murer H (2003) Disorders of renal tubular phosphate transport. J Am Soc Nephrol 14:240–247
Kronenberg HM (2002) NPT2a—The key to phosphate homeostasis. N Eng J Med 347:1022–1024
Takeda E, Yamamoto H, Nashiki K, Sato T, Arai H, Taketani Y (2004) Inorganic phosphate homeostasis and the role of dietary phosphorus. J Cell Mol Med 8:191–201
Nenet-Pages A, Lorenz-Depiereux B, Zischka H, White KE, Econs MJ, Strom TM (2004) FGF-23 is processed by proprotein convertase but not by PHEX. Bone 35:455–462
Liu S, Guo R, Simpson LG, Kiao ZS, Burnham CE, Quarles LD (2003) Regulation of fibroblastic growth factor 23 expression but not degradation by PHEX. J Biol Chem 278(39):37419–37426
White KE, Carn GC, Lorenz-Depiereux B, Benet-Pages A, Strom TM, Econs MJ (2001) Autosomal-dominant hypophosphatemic rickets (ADHR) mutations stabilize FGF-23. Kidney Int 60:2079–2086
Bowe AE, Finnegan R, Beur SMJ, Cho J, Levine MA, Kumar R, Schiavi SC (2001) FGF-23 inhibits renal tubular phosphate transport and is a PHEX substrate. Biochem Biophys Res Commun 284:977–981
Quarles LD (2003) FGF-23, PHEX and MEPE regulation of phosphate homeostasis and skeletal mineralization. Am J Physiol Endocrinol Metab 285:E1–E9
Kruse A, Dracht U, Gopfert G (1982) Renal threshold phosphate concentration (TmPO4/GFR) Arch Dis Child 57:217–223
Brodehl J, Krause A, Hoyer P (1988) Assessment of maximal tubular phosphate reabsorption: Comparison of direct measurement with the nomogram of Bijvoet. Pediatr Nephrol 2:183–189
Patriquin H, Robitaille P (1986) Renal calcium deposition in children: sonographic demonstration of the Anderson-Carr progression. AJR Am J Roentgenol 146:1253–1256
Kooh SW, Binet A, Daneman A (1994) Nephrocalcinosis in X-linked hypophosphatemic rickets: its relationship to treatment, kidney function, and growth. Clin Invest Med 17:123–130
Friedman NE, Lobaugh B, Drezner MK (1993) Effects of calcitriol and phosphorus therapy on the growth of patients with X-linked hypophosphatemia. J Clin Endocrinol Metab 76:839–844
Doria A, Kooh SW, Cole WG, Daneman A, Sochett E (2003) Early treatment improves growth and biochemical and radiographic outcome in X-linked hypophosphatemic rickets. J Clin Endocrinol Metab 88:3591–3597
Patzer L, van’t Hoff W, Shah V, Hallson P, Kasidas GP, Samuell C, de Bruyn R, Barrat TM, Dillon MJ (1999) Urinary supersaturation of calcium oxalate and phosphate in patients with X-linked hypophosphatemic rickets and in healthy schoolchildren. J Pediatr 135:611–617
Reusz GS, Latta K, Hoyer PF, Byrd DJ, Ehrich JH, Brodehl J (1990) Evidence suggesting hyperoxaluria as a cause of nephrocalcinosis in phosphate-treated rickets. Lancet 335:1240–1243
Schonaue E, Kruse K, Bohles HJ, Sewell AC (1992) More evidence for hyperoxaluria in phosphate-treated X-linked familial hypophosphatemic rickets. Eur J Pediatr 151:390
Reusz GS, Hoyer PF, Lucas M, Krohn HP, Ehrich JHH, Brodehl J (1990) X-Linked hypophosphatemic: treatment, height gain, and nephrocalcinosis. Arch Dis Child 65:1125–1128
Alon U, Donaldson DL, Hellerstein S, Warady BA, Harris DJ (1992) Metabolic and histologic investigation of the nature of nephrocalcinosis in children with hypophosphatemic rickets and in the Hyp mouse. J Pediatr 120:899–905
Goodyer PR, Kronick JB, Jequier S, Reade TM, Scriver CR (1987) Nephrocalcinosis and its relationship to treatment of hereditary rickets. J Pediatr 111:700–704
Verge CF, Lam A, Simpson JM, Cowell CT, Hoeard NJ, Silink M (1991) Effects of therapy in X-linked hypophosphatemic rickets. N Eng J Med 325:1843–1848
Seikaly M, Browne R, Baum M (1996) Nephrocalcinosis is associated with renal tubular acidosis in children with X-linked hypophosphatemia. Pediatrics 97:91–93
Minari M, Castellani A, Garella S (1984) Renal tubular acidosis associated with vitamin D-resistant rickets. Miner Electrolyte Metab 10:371–374
Saggese G, Baroncelli GI, Bertelloni S, Perri G (1995) Long-term growth hormone treatment in children with renal hypophosphatemic rickets: Effects on growth, mineral metabolism, and bone density. J Pediatr 127:395–402
Baroncelli GI, Bertelloni S, Ceccarelli C, Saggese G (2001) Effect of growth hormone treatment on final height, phosphate metabolism, and bone mineral density in children with X-linked hypophosphatemic rickets. J Pediatr 138:236–243
Reusz GS, Miltenyi G, Stubnya G, Szabo A, Horvath C, Byrd DJ, Peter F, Tulassay T (1997) X-linked hyperphosphatemia: effects of treatment with recombinant human growth hormone. Pediatr Nephrol 11:573–577
Haffner D, Wuhl E, Blum WF, Schaefer F, Mehls O (1995) Disproportionate growth following long-term growth hormone treatment in short children with X-linked hypophosphatemia. Eur J Pediatr 154:610–613
Nissel R, Wuhl E, Mehls O (2004) Effects of growth hormone treatment on body proportions and final height among small children with X-linked hypophosphatemic rickets. Pediatrics 113:e593–596
Scott A, Rivkees AS, El-Hajj-Fuleihan G, Brown EM, Crawford JD (1992) Tertiary hyperparathyroidism during high phosphate therapy of familial hypophosphatemic rickets. J Clin Endocrinol Metab 75:1514–1518
Gosnell JE, Posen S, Reeve TS, Delbridge LW (2004) Parathyroidectomy for tertiary hyperparathyroidism associated with X-linked dominant hypophosphatemic rickets. Arch Surg 139:218–222
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vaisbich, M.H., Koch, V.H. Hypophosphatemic rickets: results of a long-term follow-up. Pediatr Nephrol 21, 230–234 (2006). https://doi.org/10.1007/s00467-005-2077-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-005-2077-4