
Abstract
Background
For small to medium-sized ventral hernias, robotic intraperitoneal onlay mesh (rIPOM) and enhanced-view totally extraperitoneal (eTEP) repair have emerged as acceptable approaches that each takes advantage of robotic instrumentation. We hypothesized that avoiding mesh fixation in a robotic eTEP repair offers an advantage in early postoperative pain compared to rIPOM.
Methods
This is a multi-center, randomized clinical trial for patients with midline ventral hernias ≤ 7 cm, who were randomized to rIPOM or robotic eTEP. The primary outcome was pain (0–10) on the first postoperative day. Secondary outcomes included same-day discharge, length of stay, opioid consumption, quality of life, surgeon workload, and cost.
Results
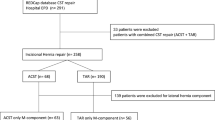
Between November 2019 and November 2021, 100 patients were randomized (49 rIPOM, 51 eTEP) among 5 surgeons. Pain on the first postoperative day [median (IQR): 5 (4–6) vs. 5 (3.5–7), p = 0.66] was similar for rIPOM and eTEP, respectively, a difference maintained following adjustments for surgeon, operative time, baseline pain, and patient co-morbidities (difference 0.28, 95% CI − 0.63 to 1.19, p = 0.56). No differences in pain on the day of surgery, 7, and 30 days after surgery were identified. Same-day discharge, length of stay, opioid consumption, and 30-day quality of life were also comparable, though rIPOM required less surgeon workload (p < 0.001), shorter operative time [107 (86–139) vs. 165 (129–212) min, p < 0.001], and resulted in fewer surgical site occurrences (0 vs. 8, p = 0.004). The total direct costs for rIPOM and eTEP were comparable [$8282 (6979–11835) vs. $8680 (7550–10282), p = 0.52] as the cost savings for eTEP attributable to mesh use [$442 (434–485) vs. $69 (62–76), p = < 0.0001] were offset by increased expenses for operative time [$669 (579–861) vs. $1075 (787–1367), p < 0.0001] and use of more robotic equipment [$760 (615–933) vs. $946 (798–1203), p = 0.001].
Conclusion
The avoidance of fixation in a robotic eTEP repair did not reveal a benefit in postoperative pain to offset the shorter operative time and surgeon workload offered by rIPOM.





Similar content being viewed by others


References
Sheetz KH, Claflin J, Dimick JB (2020) Trends in the adoption of robotic surgery for common surgical procedures. JAMA Netw Open 3:e1918911
Allison N, Tieu K, Snyder B, Pigazzi A, Wilson E (2012) Technical feasibility of robot-assisted ventral hernia repair. World J Surg 36:447–452
Belyansky I, Daes J, Radu VG, Balasubramanian R, Reza Zahiri H, Weltz AS, Sibia US, Park A, Novitsky Y (2018) A novel approach using the enhanced-view totally extraperitoneal (eTEP) technique for laparoscopic retromuscular hernia repair. Surg Endosc 32:1525–1532
Stoppa RE (1989) The treatment of complicated groin and incisional hernias. World J Surg 13:545–554
Eker HH, Hansson BM, Buunen M, Janssen IM, Pierik RE, Hop WC, Bonjer HJ, Jeekel J, Lange JF (2013) Laparoscopic vs. open incisional hernia repair: a randomized clinical trial. JAMA Surg 148:259–263
Li J, Wang Y, Wu L (2022) The comparison of eTEP and IPOM in ventral and incisional hernia repair: a systematic review and meta-analysis. Surg Laparosc Endosc Percutan Tech 32:252–258
Jain M, Krishna A, Prakash O, Kumar S, Sagar R, Ramachandran R, Bansal VK (2022) Comparison of extended totally extra peritoneal (eTEP) vs. intra peritoneal onlay mesh (IPOM) repair for management of primary and incisional hernia in terms of early outcomes and cost effectiveness—a randomized controlled trial. Surg Endosc 2022:1–9
Kumar N, Palanisamy NV, Parthasarathi R, Sabnis SC, Nayak SK, Palanivelu C (2021) A comparative prospective study of short-term outcomes of extended view totally extraperitoneal (e-TEP) repair versus laparoscopic intraperitoneal on lay mesh (IPOM) plus repair for ventral hernia. Surg Endosc 35:5072–5077
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG (2009) Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 42:377–381
Breivik EK, Bjornsson GA, Skovlund E (2000) A comparison of pain rating scales by sampling from clinical trial data. Clin J Pain 16:22–28
Cella D, Yount S, Rothrock N, Gershon R, Cook K, Reeve B, Ader D, Fries JF, Bruce B, Rose M, Group PC (2007) The patient-reported outcomes measurement information system (PROMIS): progress of an NIH roadmap cooperative group during its first two years. Med Care 45:S3–S11
Krpata DM, Schmotzer BJ, Flocke S, Jin J, Blatnik JA, Ermlich B, Novitsky YW, Rosen MJ (2012) Design and initial implementation of HerQLes: a hernia-related quality-of-life survey to assess abdominal wall function. J Am Coll Surg 215:635–642
Zheng B, Jiang X, Tien G, Meneghetti A, Panton ON, Atkins MS (2012) Workload assessment of surgeons: correlation between NASA TLX and blinks. Surg Endosc 26:2746–2750
Lowndes BR, Forsyth KL, Blocker RC, Dean PG, Truty MJ, Heller SF, Blackmon S, Hallbeck MS, Nelson H (2020) NASA-TLX assessment of surgeon workload variation across specialties. Ann Surg 271:686–692
Zolin SJ, Petro CC, Prabhu AS, Fafaj A, Thomas JD, Horne CM, Tastaldi L, Alkhatib H, Krpata DM, Rosenblatt S, Rosen MJ (2020) Registry-based randomized controlled trials: a new paradigm for surgical research. J Surg Res 255:428–435
Olavarria OA, Bernardi K, Shah SK, Wilson TD, Wei S, Pedroza C, Avritscher EB, Loor MM, Ko TC, Kao LS, Liang MK (2020) Robotic versus laparoscopic ventral hernia repair: multicenter, blinded randomized controlled trial. BMJ 370:m2457
Petro CC, Zolin S, Krpata D, Alkhatib H, Tu C, Rosen MJ, Prabhu AS (2021) Patient-reported outcomes of robotic vs. laparoscopic ventral hernia repair with intraperitoneal mesh: the PROVE-IT randomized clinical trial. JAMA Surg 156:22–29
Plymale MA, Davenport DL, Walsh-Blackmore S, Hess J, Griffiths WS, Plymale MC, Totten CF, Roth JS (2020) Costs and complications associated with infected mesh for ventral hernia repair. Surg Infect (Larchmt) 21:344–349
Kokotovic D, Bisgaard T, Helgstrand F (2016) Long-term recurrence and complications associated with elective incisional hernia repair. JAMA 316:1575–1582
Halm JA, de Wall LL, Steyerberg EW, Jeekel J, Lange JF (2007) Intraperitoneal polypropylene mesh hernia repair complicates subsequent abdominal surgery. World J Surg 31:423–429 (Discussion 430)
Gray SH, Vick CC, Graham LA, Finan KR, Neumayer LA, Hawn MT (2008) Risk of complications from enterotomy or unplanned bowel resection during elective hernia repair. Arch Surg 143:582–586
Zolin SJ, Fafaj A, Krpata DM (2020) Transversus abdominis release (TAR): What are the real indications and where is the limit? Hernia 24:333–340
Petro CC, Posielski NM, Raigani S, Criss CN, Orenstein SB, Novitsky YW (2015) Risk factors for wound morbidity after open retromuscular (sublay) hernia repair. Surgery 158:1658–1668
Albino FP, Patel KM, Nahabedian MY, Sosin M, Attinger CE, Bhanot P (2013) Does mesh location matter in abdominal wall reconstruction? A systematic review of the literature and a summary of recommendations. Plast Reconstr Surg 132:1295–1304
Warren J, Desai SS, Boswell ND, Hancock BH, Abbad H, Ewing JA, Carbonell AM, Cobb WS (2020) Safety and efficacy of synthetic mesh for ventral hernia repair in a contaminated field. J Am Coll Surg 230:405–413
Funding
Funding was provided by Society of American Gastrointestinal and Endoscopic Surgeons (Grant No. SAGES 2020 Robotic Research Grant Recipient) and Americas Hernia Society Foundation (Grant No. 2020 ACHQC Foundation Research Grant).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Clayton C. Petro has received societal research grants from the American Hernia Society and SAGES for this trial. Separate societal research grants from the American Hernia Society and Central Surgical Associations were received for other projects. Katherine C. Montelione, MD, MS—No Disclosures. Samuel J. Zolin, MD—No Disclosures. David B. Renton, MD FACS—No Disclosures. Jonathan P. Yunis, MD FACS—No Disclosures. Michael P. Meara, MD FACS—Is a paid speaker for Intuitive Surgical. Adele Costanzo, RN—No Disclosures. Kayla Diaz, MCR CCRP—No Disclosures. Kristen McKenzie, BSN RN—No Disclosures. Melanie Wilber, LPN—No Disclosures. Tamela Fonseca, MSN, RN, CCRC, NE-BC—No Disclosures. Chao Tu, MS—No Disclosures. Molly A. Olson, MS—No Disclosures. The ACHQC has contracted with Weill Cornell Medicine to provide biostatistical support for ACHQC projects. The work provided for this manuscript was performed under the umbrella of the Weill Cornell Medicine and ACHQC collaboration plan. David M. Krpata, MD FACS—No Disclosures. Lucas R. Beffa, MD FACS—Is a paid speaker for Intuitive Surgical. Ben K. Poulose, MD FACS—Has received research support from BD and Advanced Medical Solutions. He currently receives salary support from the Abdominal Core Health Quality Collaborative (ACHQC) as the Director for Quality and Outcomes. Michael J. Rosen, MD FACS—Receives salary support for role of medical director of the ACHQC, and is a board member of Ariste Medical. Ajita S. Prabhu, MD FACS—Dr. Prabhu reports research grants from Intuitive Surgical and serving as a consultant for CMR Surgical and Verb Surgical.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Petro, C.C., Montelione, K.C., Zolin, S.J. et al. Robotic eTEP versus IPOM evaluation: the REVEAL multicenter randomized clinical trial. Surg Endosc 37, 2143–2153 (2023). https://doi.org/10.1007/s00464-022-09722-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-022-09722-9