
Abstract
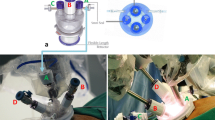
Laparoscopic distal pancreatectomy is regarded as safe and effective surgical approach in benign and low-grade malignant tumor of the pancreas. With the advances of laparoscopic techniques and instruments, many efforts to reduce the number of the trocar site has been made. There are a few available surgical techniques of laparoscopic single-site (single port or reduced port) distal pancreatectomy, suggesting its safety and feasibility. However, it is true that laparoscopic single-site distal pancreatectomy is difficult and technically quite demanding. Robotic surgical system was introduced to overcome the limitation of conventional laparoscopic surgery. Recently, we experienced robotic single-site plus ONE port distal pancreatectomy in benign and low-grade malignant tumor of the pancreas. A 45-year-old male patient was incidentally found to have pancreatic mass in tail of the pancreas. October 6th 2015, robotic distal pancreatectomy was performed using the Da Vinci single-site surgical platform (DVSSP) with one additional port. Additional robotic 12-mm-port was placed left side of DVSSP, and robotic 3rd arm was used through this site. Usual robotic instruments such as hook, bipolar, vessel sealer, and endo-GIA with endo-wrist function could be used to facilitate effective surgical procedure. The general operation procedure was based on modified Lasso technique (isolation and ligation of splenic artery prior to Lasso technique). Resected specimen was delivered through umbilicus and drains were inserted through additional port site. Five consecutive clinical experiences were reviewed. This study was approved by institutional review board. Two patients were male and three were female with median age, 38 years (range 21–56). The distribution of the pathological diagnosis was 2 solid pseudopapillary tumors, 1 serous cystic neoplasm, 1 chronic pancreatitis, and 1 neuroendocrine tumor. Median operation time was 165 min (range 120–270 min), and intraoperative-estimated blood loss were median 5 ml (range 0–50 ml). One patient could preserve spleen by Warshaw procedure. One patient converted to conventional multi-port robotic distal pancreatectomy due to inter-arms collisions. There was no clinically relevant postoperative pancreatic fistula. Length of hospital stay was median 6 days after surgery (range 5–8 days). Robotic single-site plus ONE port distal pancreatectomy is safe and feasible with acceptable perioperative outcomes. Although, certain patients such as those with a hard pancreas need an amount of care due to the features of robotic GIA, currently available robotic single-site plus ONE port surgical system was thought to have potential role to make laparoscopic single-site distal pancreatectomy much easier and ergonomics, providing some room to expand more minimally invasive surgery. Further experiences are mandatory.
Similar content being viewed by others


References
Cuschieri A (1994) Laparoscopic surgery of the pancreas. J R Coll Surg Edinb 39(3):178–184
Escobar-Dominguez JE, Hernandez-Murcia C, Gonzalez AM (2015) Description of robotic single site cholecystectomy and a review of outcomes. J Surg Oncol 112(3):284–288
Morelli L, Guadagni S, Di Franco G, Palmeri M, Di Candio G, Mosca F (2015) Da Vinci single site(c) surgical platform in clinical practice: a systematic review. Int J Med Robot. doi:10.1002/rcs.1713
de Rooij T, Klompmaker S, Hilal MA, Kendrick ML, Busch OR, Besselink MG (2016) Laparoscopic pancreatic surgery for benign and malignant disease. Nat Rev Gastroenterol Hepatol. doi:10.1038/nrgastro.2016.17
Sanchez-Cabus S, Adam JP, Pittau G, Gelli M, Cunha AS (2016) Laparoscopic left pancreatectomy: early results after 115 consecutive patients. Surg Endosc. doi:10.1007/s00464-016-4780-6
Misawa T, Ito R, Futagawa Y, Fujiwara Y, Kitamura H, Tsutsui N, Shiba H, Wakiyama S, Ishida Y, Yanaga K (2012) Single-incision laparoscopic distal pancreatectomy with or without splenic preservation: how we do it. Asian J Endosc Surg 5(4):195–199.
Machado MA, Surjan RC, Makdissi FF (2013) First single-port laparoscopic pancreatectomy in Brazil. Arq Gastroenterol 50(4):310–312
Han HJ, Yoon SY, Song TJ, Choi SB, Kim WB, Choi SY, Park SH (2014) Single-port laparoscopic distal pancreatectomy: initial experience. J Laparoendosc Adv Surg Tech A 24(12):858–863
Yao D, Wu S, Tian Y, Fan Y, Kong J, Li Y (2014) Transumbilical single-incision laparoscopic distal pancreatectomy: primary experience and review of the English literature. World J Surg 38(5):1196–1204
Kim EY, You YK, Kim DG, Lee SH, Han JH, Park SK, Na GH, Hong TH (2015) Dual-incision laparoscopic spleen-preserving distal pancreatectomy. Ann Surg Treat Res 88(3):174–177
Velanovich V (2006) The lasso technique for laparoscopic distal pancreatectomy. Surg Endosc 20(11):1766–1771
Kooby DA (2008) Laparoscopic pancreatic resection for cancer. Expert Rev Anticancer Ther 8(10):1597–1609
Acknowledgements
Some part of this contents were presented in evening seminar of the 43rd meeting of the Japanese Society of Pancreatic Surgery, Tokyo, Japan (Aug 19, 2016), and symposium of 26th World Congress of the International Association of Surgeons, Gastroenterologists, and Oncologists (IASGO, Sep 08, 2016). In addition, as corresponding author, I would like to express sincere thanks my lovely daughter, Hera Kang, for English narration embedded into this multimedia manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Dr. Sung Hyun Kim, Chang Moo Kang, and Woo Jung Lee have no conflicts of interest or financial ties to disclose.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary material 1 (MOV 254160 KB)
Rights and permissions
About this article

Cite this article
Kim, S.H., Kang, C.M. & Lee, W.J. Robotic single-site plus ONE port distal pancreatectomy. Surg Endosc 31, 4258–4259 (2017). https://doi.org/10.1007/s00464-017-5476-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-017-5476-2