
Abstract
Background
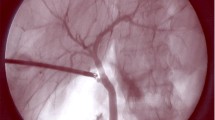
Intraoperative incisionless fluorescent cholangiography (IOIFC) has been described to identify extrahepatic biliary anatomy. Potential advantages of the routine use of intraoperative incisionless fluorescent cholangiography were evaluated in a consecutive series of cases.
Methods
A total of 45 patients undergoing laparoscopic cholecystectomy between January and July 2013 were consented and included in this study. We analyzed a prospectively collected database for feasibility, cost, time, usefulness, teaching tool, safety, learning curve, X-ray exposure, complexity, and real-time surgery of IOIFC. A single dose of 0.05 mg/kg of Indocyanine green was administered prior to surgery. During the procedure, a laparoscopic fluorescence system was used.
Results
IOIFC could be performed in all 45 patients, whereas intraoperative cholangiography could be performed in 42 (93 %). Individual median cost of performing IOFC was cheaper than IOC (13.97 ± 4.3 vs 778.43 ± 0.4 USD) per patient, p = 0.0001). IOFC was faster than IOC (0.71 ± 0.26 vs 7.15 ± 3.76 minutes, p < 0.0001). The cystic duct was identified by IOFC in 44 out of 45 patients (97.77 %).
Conclusion
IOIFC appears to be a feasible, low-cost, expeditious, useful, and effective imaging modality when performing LC. It is safe, easy to perform and interpret, and does not require a learning curve or X-ray. It can be used for real time surgery to delineate the extrahepatic biliary structures


Similar content being viewed by others


References
Niwa UC, Axt S, Falch C, Müller S, Kreuzer JA, Nedela P, Kirschniak A (2013) Laparoscopic cholecystectomy as standardised teaching operation to treat symptomatic cholecystolithiasis. Zentralbl Chir 138(2):141–142
Grbas H, Kunisek L, Zelic M, Petrosic N, Pirjavec A, Lovasic F, et al. Outcome Evaluation of 10317 Laparoscopic Cholecystectomies: A 17-Year Experience at a Single Center. Hepatogastroenterology. 2013. Epub ahead of print.
Strasberg SM, Hertl M, Soper NJ (1995) An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg 180(1):101–125
Berci G, Hunter J, Morgenstern L, Arregui M, Brunt M, Carroll B et al (2013) Laparoscopic cholecystectomy: first, do no harm; second, take care of bile duct stones. Surg Endosc 27(4):1051–1054
Yamashita Y, Kimura T, Matsumoto S (2010) A safe laparoscopic cholecystectomy depends upon the establishment of a critical view of safety. Surg Today 40(6):507–513
Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T (2003) Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA 289(13):1639–1644
Mirizzi P (1950) Operative cholangiography. Rev Esp Enferm Apar Dig Nutr. 9(3):306–308
Ido K, Isoda N, Kawamoto C, Suzuki T, Ioka T, Nagamine N et al (1996) Confirmation of a “safety zone” by intraoperative cholangiography during laparoscopic cholecystectomy. Surg Endosc 10(8):798–800
Ishizawa T, Bandai Y, Kokudo N (2009) Fluorescent cholangiography using indocyanine green for laparoscopic cholecystectomy: an initial experience. Arch Surg 144(4):381–382
Figueiredo JL, Siegel C, Nahrendorf M, Weissleder R (2010) Intraoperative near-infrared fluorescent cholangiography (NIRFC) in mouse models of bile duct injury. World J Surg 34(2):336–343
Alander T, Kaartinen I, Laakso A, Pätilä T, Spillmann T, Tuchin VV et al (2012) A review of indocyanine green fluorescent imaging in surgery. Int J Biomed Imaging 2012:940585
Takase S, Takada A, Matsuda Y (1982) Studies on the pathogenesis of the constitutional excretory defect of indocyanine green. Gastroenterologia Japonica 17(4):301–309
Litynski GS (1998) Erich Mühe and the rejection of laparoscopic cholecystectomy (1985): a surgeon ahead of his time. JSLS 2(4):341–346
Phillips EH, Berci G, Carroll B, Daykhovsky L, Sackier J, Paz-Partlow M (1990) The importance of intraoperative cholangiography during laparoscopic cholecystectomy. Am Surg 56(12):792–795
Berney CR (2012) Major common bile duct injury and risk of litigation: a surgeon’s perspective. Am J Surg 204(5):800–802
Dip FD, Asbun D, Rosales-Velderrain A, Menzo EL, Simpfendorfer CH, Szomstein S et al (2014) Cost analysis and effectiveness comparing the routine use of intraoperative fluorescent cholangiography with fluoroscopic cholangiogram in patients undergoing laparoscopic cholecystectomy. Surg Endosc 28(6):1838–1843
Way LW, Stewart L, Gantert W, Liu K, Lee CM, Whang K et al (2003) Causes and prevention of laparoscopic bile duct injuries: analysis of 252 cases from a human factors and cognitive psychology perspective. Ann Surg 237(4):460–469
Meyers WC, Peterseim DS, Pappas TN, Schauer PR, Eubanks S, Murray E et al (1996) Low insertion of hepatic segmental duct VII-VIII is an important cause of major biliary injury or misdiagnosis. Am J Surg 171(1):187–191
Sheffield KM, Han Y, Kuo YF, Townsend CM Jr, Goodwin JS, Riall TS (2012) Variation in the use of intraoperative cholangiography during cholecystectomy. J Am Coll Surg 214(4):668–679
Metcalfe MS, Ong T, Bruening MH, Iswariah H, Wemyss-Holden SA, Maddern GJ (2004) Is laparoscopic intraoperative cholangiogram a matter of routine? Am J Surg 187(4):475–481
Phillips EH, Rosenthal RJ, Carroll BJ, Fallas MJ (1994) Laparoscopic trans-cystic-duct common-bile-duct exploration. Surg Endosc 8(12):1389–1393
Lucas SM, Zeltser IS, Bensalah K, Tuncel A, Jenkins A, Pearle MS et al (2008) Training on a virtual reality laparoscopic simulator improves performance of an unfamiliar live laparoscopic procedure. J Urol 180(6):2588–2591
Singer G (2005) Occupational radiation exposure to the surgeon. J Am Acad Orthop Surg 13(1):69–76
Hope WW, Bools L, Hooks WB 3rd, Adams A, Kotwall CA, Clancy TV (2013) Teaching cholangiography in a surgical residency program. J Surg Educ 70(2):243–247
Disclosures
This study was made possible by an educational Grant from Karl Storz Endoscopy. Doctors Fernando Dip, Mayank Roy, Emanuele Lo Menzo, Conrad Simpfendorfer, Samuel Szomstein, and Raul Rosenthal have no additional disclosures.
Fundings
Funding and equipment from Karl Storz, Tuttlingen, Germany.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dip, F., Roy, M., Menzo, E.L. et al. Routine use of fluorescent incisionless cholangiography as a new imaging modality during laparoscopic cholecystectomy. Surg Endosc 29, 1621–1626 (2015). https://doi.org/10.1007/s00464-014-3853-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-014-3853-7