
Summary
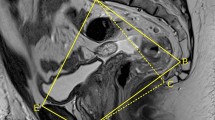
Pelvic anatomy and tumour features play a role in the difficulty of the laparoscopic approach to total mesorectal excision in rectal cancer. The aim of the study was to analyse whether these characteristics also influence the quality of the surgical specimen. We performed a prospective study in consecutive patients with rectal cancer located less than 12 cm from the anal verge who underwent laparoscopic surgery between January 2010 and July 2013. Exclusion criteria were T1 and T4 tumours, abdominoperineal resections, obstructive and perforated tumours, or any major contraindication for laparoscopic surgery. Dependent variables were the circumferential resection margin (CMR) and the quality of the mesorectum. Sixty-four patients underwent laparoscopic sphincter-preserving total mesorectal excision. Resection was complete in 79.1 % of specimens and CMR was positive in 9.7 %. Univariate analysis showed tumour depth (T status) (P = 0.04) and promontorium–subsacrum angle (P = 0.02) independently predicted CRM (circumferential resection margin) positivity. Tumour depth (P < 0.05) and promontorium–subsacrum axis (P < 0.05) independently predicted mesorectum quality. Multivariate analysis identified the promontorium–subsacrum angle (P = 0.012) as the only independent predictor of CRM. Bony pelvis dimensions influenced the quality of the specimen obtained by laparoscopy. These measurements may be useful to predict which patients will benefit most from laparoscopic surgery and also to select patients in accordance with the learning curve of trainee surgeons.


Similar content being viewed by others

References
Heald RJ, Husband EM, Ryall RD (1982) The mesorectum in rectal cancer surgery—the clue to pelvic recurrence? Br J Surg 69:613–616
MacFarlane JK, Ryall RD, Heald RJ (1993) Mesorectal excision for rectal cancer. Lancet 341:457–460
Siegel R, Cuesta MA, Targarona E, Bader FG, Morino M, Corcelles R, European Association for Endoscopic Surgery (EAES) et al (2011) Laparoscopic extraperitoneal rectal cancer surgery: the clinical practice guidelines of the European Association for Endoscopic Surgery (EAES). Surg Endosc 25:2423–2440
Arezzo A, Passera R, Scozzari G, Verra M, Morino M (2013) Laparoscopy for rectal cancer reduces short-term mortality and morbidity: results of a systematic review and meta-analysis. Surg Endosc 27:1485–1502
van der Pas MH, Haglind E, Cuesta MA, Fürst A, Lacy AM, Hop WC, Bonjer HJ (2013) COlorectal cancer Laparoscopic or Open Resection II (COLOR II) Study Group Laparoscopic versus open surgery for rectal cancer (COLOR II): short-term outcomes of a randomised, phase 3 trial. Lancet Oncol. 14:210–218
Leonard D, Penninckx F, Fieuws S, Jouret-Mourin A, Sempoux C, Jehaes C et al (2010) PROCARE, a multidisciplinary Belgian Project on Cancer of the Rectum. Factors predicting the quality of total mesorectal excision for rectal cancer. Ann Surg 252:982–988
Targarona EM, Balague C, Pernas JC, Martinez C, Berindoague R, Gich I, Trias M (2008) Can we predict immediate outcome after laparoscopic rectal surgery? Multivariate analysis of clinical, anatomic, and pathologic features after 3-dimensional reconstruction of the pelvic anatomy. Ann Surg 247:642–649
Killeen T, Banerjee S, Vijay V, Al-Dabbagh Z, Francis D, Warren S (2010) Magnetic resonance (MR) pelvimetry as a predictor of difficulty in laparoscopic operations for rectal cancer. Surg Endosc 24:2974–2979
Maughan NJ, Quirke P (2003) Modern management of colorectal cancer—a pathologist’s view. Scand J Surg. 92:11–19
Birbeck KF, Macklin CP, Tiffin NJ, Parsons W, Dixon MF, Mapstone NP et al (2002) Rates of circumferential resection margin involvement vary between surgeons and predict outcomes in rectal cancer surgery. Ann Surg 235:449–457
Salerno G, Daniels IR, Brown G, Norman AR, Moran BJ, Heald RJ (2007) Variations in pelvic dimensions do not predict the risk of circumferential resection margin (CRM) involvement in rectal cancer. World J Surg 31:1313–1320
Jeyarajah S, Sutton CD, Miller AS, Hemingway D, Leicester Colorectal Specialist Group (2007) Factors that influence the adequacy of total mesorectal excision for rectal cancer. Colorectal Dis 9:808–815
Baik SH, Kim NK, Lee KY, Sohn SK, Cho CH, Kim MJ, Kim H, Shinn RK (2008) Factors influencing pathologic results after total mesorectal excision for rectal cancer: analysis of consecutive 100 cases. Ann Surg Oncol 15:721–728
García-Granero E, Faiz O, Muñoz E, Flor B, Navarro S, Faus C et al (2009) Macroscopic assessment of mesorectal excision in rectal cancer: a useful tool for improving quality control in a multidisciplinary team. Cancer 1(115):3400–3411
Laurent C, Leblanc F, Wütrich P, Scheffler M, Rullier E (2009) Laparoscopic versus open surgery for rectal cancer: long-term oncologic results. Ann Surg 250:54–61
Akagi T, Inomata M, Etoh T, Moriyama H, Yasuda K, Shiraishi N, Eshima N, Kitano S (2012) Multivariate evaluation of the technical difficulties in performing laparoscopic anterior resection for rectal cancer. Surg Laparosc Endosc Percutan Tech. 22:52–57
Enker WE, Merchant N, Cohen AM, Lanouette NM, Swallow C, Guillem J et al (1999) Safety and efficacy of low anterior resection for rectal cancer: 681 consecutive cases from a specialty service. Ann Surg 230:544–552
Law WL, Chu KW (2004) Anterior resection for rectal cancer with mesorectal excision: a prospective evaluation of 622 patients. Ann Surg 240:260–268
Brannigan AE, De Buck S, Suetens P, Penninckx F, D’Hoore A (2006) Intracorporeal rectal stapling following laparoscopic total mesorectal excision: overcoming a challenge. Surg Endosc 20:952–955
Akiyoshi T, Kuroyanagi H, Oya M, Konishi T, Fukuda M, Fujimoto Y, Ueno M, Miyata S, Yamaguchi T (2009) Factors affecting the difficulty of laparoscopic total mesorectal excision with double stapling technique anastomosis for low rectal cancer. Surgery. 146:483–489
Bretagnol F, Lelong B, Laurent C, Moutardier V, Rullier A, Monges G (2005) The oncological safety of laparoscopic total mesorectal excision with sphincter preservation for rectal carcinoma. Surg Endosc 19:892–896
Biondo S, Ortiz H, Lujan J, Codina-Cazador A, Espin E, Garcia-Granero E, Kreisler E, de Miguel M, Alos R, Echeverria A (2010) Quality of mesorectum after laparoscopic resection for rectal cancer—results of an audited teaching programme in Spain. Colorectal Dis 12:24–31
Kim JY, Kim YW, Kim NK, Hur H, Lee K, Min BS, Cho HJ (2011) Pelvic anatomy as a factor in laparoscopic rectal surgery: a prospective study. Surg Laparosc Endosc Percutan Tech. 21:334–339
Ogiso S, Yamaguchi T, Hata H, Fukuda M, Ikai I, Yamato T, Sakai Y (2011) Evaluation of factors affecting the difficulty of laparoscopic anterior resection for rectal cancer: “narrow pelvis” is not a contraindication. Surg Endosc 25:1907–1912
Garlipp B, Ptok H, Schmidt U, Stübs P, Scheidbach H, Meyer F, Gastinger I, Lippert H (2012) Factors influencing the quality of total mesorectal excision. Br J Surg 99:714–720
Rullier A, Gourgou-Bourgade S, Jarlier M, Bibeau F, Chassagne-Clément C, Hennequin C et al (2013) Predictive factors of positive circumferential resection margin after radiochemotherapy for rectal cancer: the French randomised trial ACCORD12/0405 PRODIGE 2. Eur J Cancer 49:82–89
Veenhof AA, Engel AF, van der Peet DL, Sietses C, Meijerink WJ, de Lange-de Klerk ES, Cuesta MA (2005) Technical difficulty grade score for the laparoscopic approach of rectal cancer: a single institution pilot study. Int J Colorectal Dis 23:469–475
Leroy J, Jamali F, Forbes L, Smith M, Rubino F, Mutter D, Marescaux J (2004) Laparoscopic total mesorectal excision (TME) for rectal cancer surgery: long-term outcomes. Surg Endosc 18(281–9):60–68
Dulucq JL, Wintringer P, Stabilini C, Mahajna A (2005) Laparoscopic rectal resection with anal sphincter preservation for rectal cancer: long-term outcome. Surg Endosc 19:1468–1474
Baek SK, Carmichael JC, Pigazzi A (2013) Robotic surgery: colon and rectum. Cancer J 19:140–146
Rouanet P, Mourregot A, Azar CC, Carrere S, Gutowski M, Quenet F, Saint-Aubert B, Colombo PE (2013) Transanal endoscopic proctectomy: an innovative procedure for difficult resection of rectal tumors in men with narrow pelvis. Dis Colon Rectum 56:408–415
Acknowledgments
The authors thank Ms. C. Newey for her help and support in the English language revision of this article. This study has been supported by a Grant of Instituto de Salud Carlos III (File number: PS09/1437).
Disclosure
Authors Sonia Fernández Ananín, Eduardo M Targarona, Carmen Martinez, Juan Carlos Pernas, Diana Hernández, Ignasi Gich, Francesc J. Sancho and Manuel Trias have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Fernández Ananín, S., Targarona, E.M., Martinez, C. et al. Predicting the pathological features of the mesorectum before the laparoscopic approach to rectal cancer. Surg Endosc 28, 3458–3466 (2014). https://doi.org/10.1007/s00464-014-3622-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-014-3622-7