
Abstract
Background
Colonoscopic perforation (CP) has a low incidence rate. However, with the extensive use of colonoscopy, even low incidence rates should be evaluated to identify and address risks. Information on CP is quite limited in China.
Objective
Our study aimed to determine the frequency of CP in colonoscopies performed by surgeons at a large teaching hospital in China over a 12-year period.
Methods
A retrospective review of medical records was performed for all patients who had CPs from 1 January 2000 to 31 December 2012. Iatrogenic perforations were identified mainly by abdominal X-ray or computed tomography scan. Follow-up information of adverse events post-colonoscopy was identified from the colorectal surgery database of our hospital. Patients’ demographic data, colonoscopy procedure information, location of perforation, treatment, and outcome were recorded.
Results
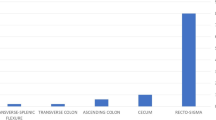
A total of 110,785 diagnostic and therapeutic colonoscopy procedures were performed (86,800 diagnostic cases and 23,985 therapeutic cases) within the 12-year study period. A total of 14 incidents (0.012 %) of CP were reported (seven males and seven females), of which nine cases occurred during diagnostic colonoscopy (0.01 %) and five after therapeutic colonoscopy (three polypectomy cases, one endoscopic mucosal resection, and one endoscopic mucosal dissection). Mean patient age was 67.14 years. One case of CP (7.14 %) after colonoscopy polypectomy was treated using curative colonoscopy endoclips. Other patients underwent operations: six cases (46.15 %) of primary repair, four cases (28.57 %) of resection with anastomosis, and two cases (15.38 %) of resection without anastomosis. No obvious perforation was found in one patient (7.69 %). Surgeons attempted to treat one case laparoscopically but eventually resorted to open surgery. The postoperative course was uncomplicated in eight cases (57.14 %) and complicated in six cases (42.86 %) but without mortality.
Conclusion
CP is a serious but rare complication of colonoscopy. A perforation risk of 0.012 % was found in our study. The optimal management of CP remains controversial. Treatment for CP should be individualized according to the patient’s condition, related devices, and surgical skills of endoscopists or surgeons. Selective measures such as colonoscopy without intravenous sedation and decrease of loop formation can effectively reduce rates of perforation.
Similar content being viewed by others


References
Wolff WI, Shinya H (1971) Colonofiberoscopy. JAMA 217:1509–1512
Avgerinos DV, Liaguna OH, Lo AY et al (2008) Evolving management of colonoscopic perforations. J Gastrointest Surg 12:1783–1789
US Preventive Services Task Force (2008) Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. Ann Intern Med 149:627–637
McFarland EG, Levin B, Lieberman DA et al (2008) Revised colorectal screening guidelines: joint effort of the American Cancer Society, US Multisociety Task Force on Colorectal Cancer, and American College of Radiology. Radiology 248:717–720
Gerstenberger PD, Plumeri PA (1993) Malpractice claims in gastrointestinal endoscopy: analysis of an insurance industry data base. Gastrointest Endosc 39:132–138
Anderson ML, Pasha TM, Leighton JA (2000) Endoscopic perforation of the colon: lessons from a 10-year study. Am J Gastroenterol 95:3418–3422
Nelson DB, McQuaid KR, Bond JH et al (2002) Procedural success and complications of large-scale screening colonoscopy. Gastrointest Endosc 55:307–314
Garbay JR, Suc B, Rotman N et al (1996) Multicentre study of surgical complications of colonoscopy. Br J Surg 83:42–44
Jentschura D, Raute M, Winter J et al (1994) Complications in endoscopy of the lower gastrointestinal tract. Therapy and prognosis. Surg Endosc 8:672–676
Tran DQ, Rosen L, Kim R et al (2001) Actual colonoscopy: what are the risks of perforation? Am Surg 67:845–847
Lüning TH, Keemers ME, Barendregt WB et al (2007) Colonoscopic perforations: a review of 30,366 patients. Surg Endosc 21:994–997
Rex DK, Bond JH, Winawer S et al (2002) Quality in the technical performance of colonoscopy and the continuous quality improvement process for colonoscopy: recommendations of the U.S. Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol 97:1296–1308
American Society for Gastrointestinal Endoscopy (2003) Complications of colonoscopy. Gastrointest Endosc 57:441–445
Araghizadeh FY, Timmcke AE, Opelka FG et al (2001) Colonoscopic perforations. Dis Colon Rectum 44:713–716
Sieg A, Hachmoeller EU, Eisenbach T (2001) Prospective evaluation of complications in outpatient GI endoscopy: a survey among German gastroenterologists. Gastrointest Endosc 53:620–627
Gatto NM, Frucht H, Sundararajan V et al (2003) Risk of perforation after colonoscopy and sigmoidoscopy: a population-based study. J Natl Cancer Inst 95:230–236
Korman LY, Overholt BF, Box T et al (2003) Perforation during colonoscopy in endoscopic ambulatory surgical centers. Gastrointest Endosc 58:554–557
Cobb WS, Heniford BT, Sigmon LB et al (2004) Colonoscopic perforations: incidence, management, and outcomes. Am Surg 70:750–757 discussion 757–758
Iqbal CW, Chun YS, Farley DR (2005) Colonoscopic perforations: a retrospective review. J Gastrointest Surg 9:1229–1235
Rabeneck L, Paszat LF, Hilsden RJ et al (2008) Bleeding and perforation after outpatient colonoscopy and their risk factors in usual clinical practice. Gastroenterology 135:1899–1906
Iqbal CW, Cullinane DC, Schiller HJ et al (2008) Surgical management and outcomes of 165 colonoscopic perforations from a single institution. Arch Surg 143:701–706 discussion 706–707
Teoh AY, Poon CM, Lee JF et al (2009) Outcomes and predictors of mortality and stoma formation in surgical management of colonoscopic perforations: a multicenter review. Arch Surg 144:9–13
Arora G, Mannalithara A, Singh G et al (2009) Risk of perforation from a colonoscopy in adults: a large population-based study. Gastrointest Endosc 69:654–664
Mai CM, Wen CC, Wen SH et al (2010) Iatrogenic colonic perforation by colonoscopy: a fatal complication for patients with a high anesthetic risk. Int J Colorectal Dis 25:449–454
Rabeneck L, Saskin R, Paszat LF (2011) Onset and clinical course of bleeding and perforation after outpatient colonoscopy: a population-based study. Gastrointest Endosc 73:520–523
Dafnis G, Ekbom A, Pahlman L et al (2001) Complications of diagnostic and therapeutic colonoscopy within a defined population in Sweden. Gastrointest Endosc 54:302–309
Lohsiriwat V, Sujarittanakarn S, Akaraviputh T et al (2008) Colonoscopic perforation: a report from World Gastroenterology Organization endoscopy training center in Thailand. World J Gastroenterol 14:6722–6725
Gedebou TM, Wong RA, Rappaport WD et al (1996) Clinical presentation and management of iatrogenic colon perforations. Am J Surg 172:454–457 discussion 457–458
Lohsiriwat V, Sujarittanakarn S, Akaraviputh T et al (2009) What are the risk factors of colonoscopic perforation? BMC Gastroenterol 9:71
Trecca A, Gaj F, Gagliardi G (2008) Our experience with endoscopic repair of large colonoscopic perforations and review of the literature. Tech Coloproctol 12:315–321
Day LW, Kwon A, Inadomi JM et al (2011) Adverse events in older patients undergoing colonoscopy: a systematic review and meta-analysis. Gastrointest Endosc 74:885–896
Karajeh MA, Sanders DS, Hurlstone DP (2006) Colonoscopy in elderly people is a safe procedure with a high diagnostic yield: a prospective comparative study of 2000 patients. Endoscopy 38:226–230
Saunders BP, Fukumoto M, Halligan S et al (1996) Why is colonoscopy more difficult in women? Gastrointest Endosc 43:124–126
Ramirez FC (2012) Re-learning colonoscopy: just a matter of time. J Interv Gastroenterol 2(3):133–134
Rodney WM, Dabov G, Orientale E et al (1993) Sedation associated with a more complete colonoscopy. J Fam Pract 36:394–400
Radaelli F, Meucci G, Sgroi G, Italian Association of Hospital Gastroenterologist (AIGO) (2008) Technical performance of colonoscopy: the key role of sedation/analgesia and other quality indicators. Am J Gastroenterol 103:1122–1130
Johannes L (2011) The patient’s perspective: patients should be made aware of the options of sedation or no sedation and have a choice in screening colonoscopy. J Interv Gastroenterol 1(1):42–44
Putcha RV, Burdick JS (2003) Management of iatrogenic perforation. Gastroenterol Clin N Am 32:1289–1309
Choo WK, Subhani J (2012) Complication rates of colonic polypectomy in relation to polyp characteristics and techniques: a district hospital experience. J Interv Gastroenterol 2(1):8–11
Zissin R, Konikoff F, Gayer G (2006) CT findings of latrogenic complications following gastrointestinal endoluminal procedures. Semin Ultrasound CT MR 27:126–138
Kim DH, Pickhardt PJ, Taylor AJ et al (2008) Imaging evaluation of complications at optical colonoscopy. Curr Probl Diagn Radiol 37:165–177
Yoshikane H, Hidano H, Sakakibara A et al (1997) Endoscopic repair by clipping of iatrogenic colonic perforation. Gastrointest Endosc 46:464–466
Lohsiriwat V (2010) Colonoscopic perforation: incidence, risk factors, management and outcome. World J Gastroenterol 16:425–430
Jovanovic I, Zimmermann L, Fry LC et al (2011) Feasibility of endoscopic closure of an iatrogenic colon perforation occurring during colonoscopy. Gastrointest Endosc 73:550–555
Siegel D (2013) Changes in colonoscopy: new tricks for an old dog. J Interv Gastroenterol 3(2):57–58
Wullstein C, Koppen M, Gross E (1999) Laparoscopic treatment of colonic perforations related to colonoscopy. Surg Endosc 13:484–487
Hansen AJ, Tessier DJ, Anderson ML et al (2007) Laparoscopic repair of colonoscopic perforations: indications and guidelines. J Gastrointest Surg 11:655–659
Alonso S, Dorcaratto D, Pera M et al (2010) Incidence of iatrogenic perforation during colonoscopy and their treatment in a university hospital. Cir Esp 88:41–45
Busić Z, Lovrić Z, Busić V et al (2007) Laparoscopic treatment of iatrogenic endoscopic sigmoid colon perforation: a case report and literature review. J Laparoendosc Adv Surg Tech A 17:324–325
Disclosure
Xiaohui Shi, Yongqi Shan, Enda Yu, Ronggui Meng, Miao Lin, Honglian Xu, Hantao Wang, Lianjie Liu, Liqiang Hao, Wei Zhang, Chuangang Fu, Hao Wang, Xiaodong Xu, Haifeng Gong, Zheng Lou, Junjie Xing, Xianhua Gao, Beili Cai and Haiyan He have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
Xiaohui Shi and Yongqi Shan contributed equally to the paper.
Rights and permissions
About this article
Cite this article
Shi, X., Shan, Y., Yu, E. et al. Lower rate of colonoscopic perforation: 110,785 patients of colonoscopy performed by colorectal surgeons in a large teaching hospital in China. Surg Endosc 28, 2309–2316 (2014). https://doi.org/10.1007/s00464-014-3458-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-014-3458-1