
Abstract
Background
We conducted this study to investigate how physical and cognitive ergonomic workloads would differ between robotic and laparoscopic surgeries and whether any ergonomic differences would be related to surgeons’ robotic surgery skill level. Our hypothesis is that the unique features in robotic surgery will demonstrate skill-related results both in substantially less physical and cognitive workload and uncompromised task performance.
Methods
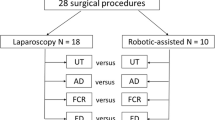
Thirteen MIS surgeons were recruited for this institutional review board-approved study and divided into three groups based on their robotic surgery experiences: laparoscopy experts with no robotic experience, novices with no or little robotic experience, and robotic experts. Each participant performed six surgical training tasks using traditional laparoscopy and robotic surgery. Physical workload was assessed by using surface electromyography from eight muscles (biceps, triceps, deltoid, trapezius, flexor carpi ulnaris, extensor digitorum, thenar compartment, and erector spinae). Mental workload assessment was conducted using the NASA-TLX.
Results
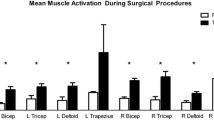
The cumulative muscular workload (CMW) from the biceps and the flexor carpi ulnaris with robotic surgery was significantly lower than with laparoscopy (p < 0.05). Interestingly, the CMW from the trapezius was significantly higher with robotic surgery than with laparoscopy (p < 0.05), but this difference was only observed in laparoscopic experts (LEs) and robotic surgery novices. NASA-TLX analysis showed that both robotic surgery novices and experts expressed lower global workloads with robotic surgery than with laparoscopy, whereas LEs showed higher global workload with robotic surgery (p > 0.05). Robotic surgery experts and novices had significantly higher performance scores with robotic surgery than with laparoscopy (p < 0.05).
Conclusions
This study demonstrated that the physical and cognitive ergonomics with robotic surgery were significantly less challenging. Additionally, several ergonomic components were skill-related. Robotic experts could benefit the most from the ergonomic advantages in robotic surgery. These results emphasize the need for well-structured training and well-defined ergonomics guidelines to maximize the benefits utilizing the robotic surgery.








Similar content being viewed by others

References
Tittiranonda P, Rempel D, Armstrong T, Burastero S (1999) Effect of four computer keyboards in computer users with upper extremity musculoskeletal disorders. Am J Ind Med 5:647–661
Andreoni G, Santambrogio GC, Rabuffetti M, Pedotti A (2002) Method for the analysis of posture and interface pressure of car drivers. Appl Ergon 33:511–522
http://iea.cc/01_what/What%20is%20Ergonomics.html (2012) What is ergonomics? Int Ergon Assoc (IEA)
DiDomenico A, Nussbaum MA (2008) Int J Indust Ergon 38:977–983
Reyes DA, Tang B, Cuschieri A (2006) Minimal access surgery (MAS)-related surgeon morbidity syndromes. Surg Endosc 20(1):1–13
Keyserling RM (1986) A computer-aided system to evaluate postural stress in the workplace. Am Ind Hyg Assoc J 47:641–649
Elhage O, Murphy D, Challacombe B, Shortland A, Dasgupta P (2007) Ergonomics in minimally invasive surgery. Int J Clin Pract 61(2):186–188A
Lee G, Lee TH, Dexter DJ, Godinez C, Meenaghan N, Catania R, Park AE (2009) Ergonomic risk of assisting in minimally invasive surgery. Surg Endosc 23(1):182–188
Park A, Lee G, Seagull FJ, Meenaghan N, Dexter D (2010) Patients benefit while surgeons suffer: an impending epidemic. J Am Coll Surg 210(3):306–313
Berguer R, Forkey DL, Smith WD (1999) Ergonomic problems associated with laparoscopic surgery. Surg Endosc 13:466–468
Lee G, Sutton E, Yassar Y, Clanton T, Park A (2011) Higher physical workload risks with NOTES versus laparoscopy: a quantitative ergonomic assessment. Surg Endosc 25(5):1585–1593
Carswell CM, Duncan C, Seales WB (2005) Assessing mental workload during laparoscopic surgery. Surg Innov 12:80–90
Lee G, Youssef Y, Carswell M, Park A (2009) Ergonomic safety of surgical techniques and standing positions associated with laparoscopic cholecystectomy. Proc Hum Factors Ergon Soc Ann Conf 53(11):723–727
Weinstein GS, O’Malley BW Jr, Desai SC, Quon H (2009) Transoral robotic surgery: does the ends justify the means? Curr Opin Otolaryngol Head Neck Surg 17(2):126–131
Boggess JF (2007) Robotic surgery in gynecologic oncology: evolution of a new surgical paradigm. J Robot Surg 1(1):31–37
O’Malley BW Jr, Weinstein GS, Snyder W, Hockstein NG (2006) Transoral robotic surgery (TORS) for base of tongue neoplasms. Laryngoscope 116(8):1465–1472
Payne TN, Dauterive FR (2008) A comparison of total laparoscopic hysterectomy to robotically assisted hysterectomy: surgical outcomes in a community practice. J Minim Invasive Gynecol 15(3):286–291
Lee EC, Rafiq A, Merrell R, Ackerman R, Dennerlein JT (2005) Ergonomics and human factors in endoscopic surgery: a comparison of manual vs. telerobotic simulation systems. Surg Endosc 19:1064–1070
Stefanidis D, Wang F, Korndorffer JR, Dunne JB, Scott DJ (2010) Robotic assistance improves intracorporeal suturing performance and safety in the operating room while decreasing operator workload. Surg Endosc 24:377–382
Stefanidis D, Hope WW, Scott DJ (2011) Robotic suturing on the FLS model possesses construct validity, is less physically demanding, and is favored by more surgeons compared with laparoscopy. Surg Endosc 25(7):2141–2146
Lawson EH, Curet MJ, Sanchez BR, Schuster R, Berguer R (2007) A comparison of robotic, laparoscopic, and hand-sewn intestinal sutured anastomoses performed by residents. Am J Surg 193(3):349–355
Berguer R, Smith W (2006) An ergonomic comparison of robotic and laparoscopic technique: the influence of surgeon experience and task complexity. J Surg Res 134:87–92
Marecik SJ, Prasad LM, Park JJ, Jan A, Chaudhry V (2008) Evaluation of midlevel and upper-level residents performing their first robotic-sutured intestinal anastomosis. Am J Surg 195(3):333–337
Klein MI, Warm JS, Riley MA, Matthews G, Doarn C, Donovan JF, Gaitonde K (2012) Mental workload and stress perceived by novice operators in the laparoscopic and robotic minimally invasive surgical interfaces. J Endourol 26(8):1089–1094
Lee G, Kavic SM, George IM, Park AE (2007) Postural instability does not necessarily correlate to poor performance: case in point. Surg Endosc 21(3):471–474
Acknowledgments
This study was supported by a clinical robotics research Grant from the 2012 Intuitive Surgical, Inc. The authors acknowledge the thoughtful and careful assistance of Elizabeth Cockey and Valerie K. Scott in editing the manuscript.
Disclosures
Dr. Gyusung Lee received 2012 Intuitive Surgical Robotic Clinical Research Grant as the Principle Investigator of this study. Drs. Mija Lee, Erica Sutton, Adrian Park, and Michael Marohn and Mrs. Tameka Clanton have no conflict of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lee, G.I., Lee, M.R., Clanton, T. et al. Comparative assessment of physical and cognitive ergonomics associated with robotic and traditional laparoscopic surgeries. Surg Endosc 28, 456–465 (2014). https://doi.org/10.1007/s00464-013-3213-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-013-3213-z