
Abstract
Background
For patients with known or suspected adrenocortical carcinoma (ACC), considerable controversy exists over the use of laparoscopic adrenalectomy. The purpose of this study was to assess recurrence and survival patterns in patients with a pathologic diagnosis of ACC treated with laparoscopic versus open adrenalectomy.
Methods
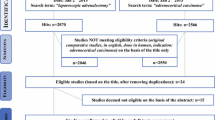
All patients referred to our center with a diagnosis of ACC from April 1, 1993 to May 1, 2012 were reviewed. Three groups of patients were compared: patients referred after laparoscopic resection elsewhere, patients referred after open resection elsewhere, and patients treated primarily at our center (all resected by the open approach). Clinical factors and overall, recurrence-free, and peritoneal recurrence-free survivals were compared between groups.
Results
During the study period, 46 patients presented after laparoscopic resection at an outside institution, 210 patients after open resection at an outside institution, and 46 patients were treated at our institution with open resection. Despite a smaller tumor size, patients treated laparoscopically developed peritoneal carcinomatosis more frequently compared to those treated with an open approach (p = 0.006 for number with peritoneal recurrence). When controlling for tumor stage, open-approach patients experienced superior recurrence-free and overall survival.
Conclusion
Despite typically being performed in patients with smaller tumors, laparoscopic adrenalectomy for ACC is associated with higher rates of recurrence, particularly peritoneal recurrence. For patients with known or suspected ACC, the oncologic benefits of open resection outweigh the short-term benefits of minimally invasive surgery.



Similar content being viewed by others


References
Lafemina J, Brennan MF (2012) Adrenocortical carcinoma: past, present, and future. J Surg Oncol 106:586–594
Grubbs EG, Callender GG, Xing Y, Perrier ND, Evans DB, Phan AT, Lee JE (2010) Recurrence of adrenal cortical carcinoma following resection: surgery alone can achieve results equal to surgery plus mitotane. Ann Surg Oncol 17:263–270
Rodgers SE, Evans DB, Lee JE, Perrier ND (2006) Adrenocortical carcinoma. Surg Oncol Clin N Am 15:535–553
Schulick RD, Brennan MF (1999) Long-term survival after complete resection and repeat resection in patients with adrenocortical carcinoma. Ann Surg Oncol 6:719–726
Eichhorn-Wharry LI, Talpos GB, Rubinfeld I (2012) Laparoscopic versus open adrenalectomy: another look at outcome using the Clavien classification system. Surgery 152:1090–1095
Lee J, El-Tamer M, Schifftner T, Turrentine FE, Henderson WG, Khuri S, Hanks JB, Inabnet WB 3rd (2008) Open and laparoscopic adrenalectomy: analysis of the National Surgical Quality Improvement Program. J Am Coll Surg 206:953–959 Discussion 959–961
Carnaille B (2012) Adrenocortical carcinoma: which surgical approach? Langenbecks Arch Surg 397:195–199
Zini L, Porpiglia F, Fassnacht M (2011) Contemporary management of adrenocortical carcinoma. Eur Urol 60:1055–1065
Gonzalez RJ, Shapiro S, Sarlis N, Vassilopoulou-Sellin R, Perrier ND, Evans DB, Lee JE (2005) Laparoscopic resection of adrenal cortical carcinoma: a cautionary note. Surgery 138:1078–1085 Discussion 1085–1076
Porpiglia F, Fiori C, Daffara F, Zaggia B, Bollito E, Volante M, Berruti A, Terzolo M (2010) Retrospective evaluation of the outcome of open versus laparoscopic adrenalectomy for stage I and II adrenocortical cancer. Eur Urol 57:873–878
Brix D, Allolio B, Fenske W, Agha A, Dralle H, Jurowich C, Langer P, Mussack T, Nies C, Riedmiller H, Spahn M, Weismann D, Hahner S, Fassnacht M, German G, Adrenocortical Carcinoma Registry (2010) Laparoscopic versus open adrenalectomy for adrenocortical carcinoma: Surgical and oncologic outcome in 152 patients. Eur Urol 58:609–615
Mir MC, Klink JC, Guillotreau J, Long JA, Miocinovic R, Kaouk JH, Simmons MN, Klein E, Krishnamurthi V, Campbell SC, Fergany AF, Reynolds J, Stephenson AJ, Haber GP (2013) Comparative outcomes of laparoscopic and open adrenalectomy for adrenocortical carcinoma: single, high-volume center experience. Ann Surg Oncol 20:1456–1461
Lombardi CP, Raffaelli M, De Crea C, Boniardi M, De Toma G, Marzano LA, Miccoli P, Minni F, Morino M, Pelizzo MR, Pietrabissa A, Renda A, Valeri A, Bellantone R (2012) Open versus endoscopic adrenalectomy in the treatment of localized (stage I/II) adrenocortical carcinoma: results of a multiinstitutional Italian survey. Surgery 152:1158–1164
Porpiglia F, Miller BS, Manfredi M, Fiori C, Doherty GM (2011) A debate on laparoscopic versus open adrenalectomy for adrenocortical carcinoma. Horm Cancer 2:372–377
Miller BS, Ammori JB, Gauger PG, Broome JT, Hammer GD, Doherty GM (2010) Laparoscopic resection is inappropriate in patients with known or suspected adrenocortical carcinoma. World J Surg 34:1380–1385
Leboulleux S, Deandreis D, Al Ghuzlan A, Auperin A, Goere D, Dromain C, Elias D, Caillou B, Travagli JP, De Baere T, Lumbroso J, Young J, Schlumberger M, Baudin E (2010) Adrenocortical carcinoma: is the surgical approach a risk factor of peritoneal carcinomatosis? Eur J Endocrinol 162:1147–1153
Sroka G, Slijper N, Shteinberg D, Mady H, Galili O, Matter I (2013) Laparoscopic adrenalectomy for malignant lesions: surgical principles to improve oncologic outcomes. Surg Endosc. doi:10.1007/s00464-012-2772-8
Kirshtein B, Yelle JD, Moloo H, Poulin E (2008) Laparoscopic adrenalectomy for adrenal malignancy: a preliminary report comparing the short-term outcomes with open adrenalectomy. J Laparoendosc Adv Surg Tech A 18:42–46
Stefanidis D, Goldfarb M, Kercher K, Hope W, Richardson W, Fanelli R (2013) Guidelines for the minimally invasive treatment of adrenal pathology. http://www.sages.org/publications/guidelines/guidelines-for-the-minimally-invasive-treatment-of-adrenal-pathology/
Barnett CC Jr, Varma DG, El-Naggar AK, Dackiw AP, Porter GA, Pearson AS, Kudelka AP, Gagel RF, Evans DB, Lee JE (2000) Limitations of size as a criterion in the evaluation of adrenal tumors. Surgery 128:973–982 Discussion 982–973
Herrera MF, Grant CS, van Heerden JA, Sheedy PF, Ilstrup DM (1991) Incidentally discovered adrenal tumors: an institutional perspective. Surgery 110:1014–1021
Graham DJ, McHenry CR (1998) The adrenal incidentaloma: guidelines for evaluation and recommendations for management. Surg Oncol Clin N Am 7:749–764
Office of Disease Prevention (2002) NIH state-of-the-science statement on management of the clinically inapparent adrenal mass (“incidentaloma”). http://consensus.nih.gov/2002/2002AdrenalIncidentalomasos021main.htm. Accessed 15 April 2013
Bharwani N, Rockall AG, Sahdev A, Gueorguiev M, Drake W, Grossman AB, Reznek RH (2011) Adrenocortical carcinoma: the range of appearances on CT and MRI. AJR Am J Roentgenol 196:W706–W714
Groussin L, Bonardel G, Silvera S, Tissier F, Coste J, Abiven G, Libe R, Bienvenu M, Alberini JL, Salenave S, Bouchard P, Bertherat J, Dousset B, Legmann P, Richard B, Foehrenbach H, Bertagna X, Tenenbaum F (2009) 18F-fluorodeoxyglucose positron emission tomography for the diagnosis of adrenocortical tumors: a prospective study in 77 operated patients. J Clin Endocrinol Metab 94:1713–1722
Acknowledgments
This research was supported in part by the National Institutes of Health through MD Anderson’s Cancer Center Support Grant (CA016672).
Disclosures
Amanda B. Cooper MD, Mouhammed Amir Habra MD, Elizabeth G. Grubbs MD, Brian K. Bednarski MD, Anita K. Ying MD, Nancy D. Perrier MD, Jeffrey E. Lee MD, and Thomas A. Aloia MD have no conflicts of interest to disclose relevant to this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cooper, A.B., Habra, M.A., Grubbs, E.G. et al. Does laparoscopic adrenalectomy jeopardize oncologic outcomes for patients with adrenocortical carcinoma?. Surg Endosc 27, 4026–4032 (2013). https://doi.org/10.1007/s00464-013-3034-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-013-3034-0