
Abstract
Background
By traditional open surgery, the tumor recurrence rate of total mesorectal excision with sphincter-preserving procedure was lower than that of abdominoperineal resection (APR) for the treatment of low rectal cancer. The present study aimed to rescrutinize whether the same conclusion can be drawn when both surgical procedures are performed laparoscopically.
Methods
We retrospectively reviewed the prospectively recorded clinicopathologic data of 344 consecutive patients with low rectal cancer, in which 170 patients underwent preoperative chemoradiotherapy followed by laparoscopic total mesorectal excision (TME), whereas 174 patients underwent laparoscopic TME directly without chemoradiotherapy. Such patients were further stratified according to the pathologic tumor, node, metastasis stage (stage II or III disease) and surgical strategy (APR or sphincter-preserving operation [SPO]). The surgical procedures are presented in supplemental videos. The disease-free survival, recurrence patterns, and functional recovery of patient groups stratified as appropriate were compared.
Results
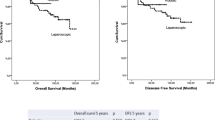
In patients who received preoperative chemoradiotherapy, the estimated recurrence rate were similar between laparoscopic TME with SPO and laparoscopic APR with 10.6 %, 7 of 66, versus 18.5 %, 5 of 27, in stage II disease (p = 0.811, log-rank test); and 19.3 %, 11 of 57, versus 20 %, 4 of 20, in stage III disease (p = 0.980). In patients without preoperative chemoradiotherapy, the recurrence rate was significantly higher in laparoscopic APR than in the laparoscopic TME with SPO group of patients with stage III disease (45 %, 9 of 20, vs. 19.3 %, 16 of 83, p = 0.025), whereas the recurrence rate of the two procedures was similar (21.4 %, 3 of 14, vs. 17.5 %, 10 of 57, p = 0.702) in stage II disease.
Conclusions
When low rectal cancer was operated on by laparoscopic approach, the poorer prognosis of APR compared to SPO was only observed in stage III patients without preoperative chemoradiotherapy.




Similar content being viewed by others


Abbreviations
- CCRT:
-
Concurrent chemoradiation therapy
- TME:
-
Total mesorectal excision
- SPO:
-
Sphincter-preserving operation
References
Heald RJ, Smedh RK, Kald A et al (1997) Abdominoperineal excision of the rectum—an endangered operation. Dis Colon Rectum 40:747–751
Law WL, Chu KW (2004) Abdominoperineal resection is associated with poor oncological outcome. Br J Surg 91:1493–1499
Marr R, Birbeck K, Garvican J et al (2005) The modern abdominoperineal excision: the next challenge after total mesorectal excision. Ann Surg 242:74–82
Nagtegaal ID, van de Velde CJ, Marijnen CA et al (2005) Low rectal cancer: a call for a change of approach in abdominoperineal resection. J Clin Oncol 23:9257–9264
Rullier E, Laurent C, Bretagnol F, Rullier A, Vendrely V, Zerbib F (2005) Sphincter-saving resection for all rectal carcinomas: the end of the 2-cm distal rule. Ann Surg 241:465–469
Simunovic M, Sexton R, Rempel E, Moran BJ, Heald RJ (2003) Optimal preoperative assessment and surgery for rectal cancer may greatly limit the need for radiotherapy. Br J Surg 90:999–1003
de Gramont A, Boni C, Navarro M et al (2007) Oxaliplatin/5FU/LV in adjuvant colon cancer: updated efficacy results of the MOSAIC trial, including survival, with a median follow-up of six years (abstract). Proceedings of ASCO
Liang JT, Lai HS, Lee PH (2007) Laparoscopic pelvic autonomic nerve-preserving surgery for patients with lower rectal cancer after chemoradiation therapy. Ann Surg Oncol 14:1285–1287
Liang JT, Lai HS, Lee PH (2006) Multimedia article. Laparoscopic abdominoperineal resection for lower rectal cancers: how do we do it? Surg Endosc 20:695–696
Liang JT, Lai HS, Lee PH (2006) Multimedia article. Laparoscopic abdominoanal pull-through procedure for male patients with lower rectal cancer after chemoradiation therapy. Dis Colon Rectum 49:259–260
Heald RJ, Moran BJ, Brown G, Daniels IR (2004) Optimal total mesorectal excision for rectal cancer is by dissection in front of Denonvilliers’ fascia. Br J Surg 91:121–123
Kinugasa Y, Murakami G, Uchimoto K et al (2006) Operating behind Denonvilliers’ fascia for reliable preservation of urogenital autonomic nerves in total mesorectal excision: a histologic study using cadaveric specimens, including a surgical experiment using fresh cadaveric models. Dis Colon Rectum 49:1024–1032
Liang JT, Lai HS, Cheng KW (2011) Laparoscopic dissection of Denonvilliers’ fascia implicated for total mesorectal excision for treatment of rectal cancer. Surg Endosc 25:935–940
Nagtegaal ID, Marijnen CA, Kranenbarg EK et al (2002) Circumferential margin involvement is still an important predictor of local recurrence in rectal carcinoma: not one millimeter but two millimeters is the limit. Am J Surg Pathol 26:350–357
Nagtegaal ID, van de Velde CJ, van der Worp E, Kapiteijn E, Quirke P, van Krieken JH, Cooperative Clinical Investigators of the Dutch Colorectal Cancer Group (2002) Macroscopic evaluation of rectal cancer resection specimen: clinical significance of the pathologist in quality control. J Clin Oncol 20:1729–1734
Liang JT, Huang KC, Lai HS, Lee PH, Sun CT (2007) Oncologic results of laparoscopic D3 lymphadenectomy for male sigmoid and upper rectal cancer with clinically positive lymph nodes. Ann Surg Oncol 14:1980–1990
Liang JT, Lai HS, Huang KC, Chang KJ, Shieh MJ, Jeng YM, Wang SM (2003) Comparison of medial-to-lateral versus traditional lateral-to-medial laparoscopic dissection sequences for resection of rectosigmoid cancers: randomized controlled clinical trial. World J Surg 27:190–196
Radcliffe A (2006) Can the results of anorectal (abdominoperineal) resection be improved: are circumferential resection margins too often positive? Colorectal Dis 8:160–167
Ahmad NZ, Racheva G, Elmusharaf H (2013) A systematic review and meta-analysis of randomized and non-randomized studies comparing laparoscopic and open abdominoperineal resection for rectal cancer. Colorectal Dis 15:269–277. doi:10.1111/codi.12007
Lee SH, Hernandez de Anda E, Finne CO et al (2005) The effect of circumferential tumor location in clinical outcomes of rectal cancer patients treated with total mesorectal excision. Dis Colon Rectum 48:2249–2257
Acknowledgments
This study was supported from National Science Council, Taiwan (NSC 96-2314-B-002-146) and Research Fund of Colorectal Cancer in National Taiwan University Hospital. The fund supported laboratory experiment and management of clinical data.
Disclosures
Jin-Tung Liang, Jason Chia-Hsien Cheng, Kuo-Chin Huang, Hong-Shiee Lai, and Chia-Tung Sun have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary material 1 (MPG 9829 kb)
Supplementary material 2 (MPG 10428 kb)
Supplementary material 3 (MPG 8889 kb)
Supplementary material 4 (MPG 10816 kb)
Rights and permissions
About this article
Cite this article
Liang, JT., Cheng, J.CH., Huang, KC. et al. Comparison of tumor recurrence between laparoscopic total mesorectal excision with sphincter preservation and laparoscopic abdominoperineal resection for low rectal cancer. Surg Endosc 27, 3452–3464 (2013). https://doi.org/10.1007/s00464-013-2898-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-013-2898-3