
Abstract
Background
Diagnostic laparoscopy is the ultimate diagnostic tool to evaluate the appendix. Still, according to the literature, this strategy results in a negative appendectomy rate of approximately 12–18 % and associated morbidity. Laparoscopic criteria for determining appendicitis are lacking. The goal of this study is to define clear and reliable criteria for appendicitis during diagnostic laparoscopy that eventually may safely reduce the negative appendectomy rate.
Methods
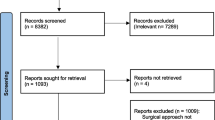
From December 2009 through April 2011, 134 patients were included and analysed in a single-centre prospective pilot study. Intraoperatively, the appendix was evaluated by the surgeon according to nine criteria for appendicitis. The operating surgeon decided whether it should be removed or not. Immediately after the operation the surgeon had to complete a questionnaire on nine criteria for appendicitis. All removed appendices were examined by a pathologist. In case the appendix was not removed, the clinical postoperative course was decisive for the (missed) presence of appendicitis.
Results
In 109 cases an inflamed appendix was removed; in 25 patients the appendix was normal, 3 of which had been removed. After univariate analysis and clinical judgement six variables were included in the Laparoscopic APPendicitis score (LAPP score). In this study, use of the LAPP score would have led to a positive predictive value of 99 % and a negative predictive value of 100 %.
Conclusions
This study presents the LAPP score. The LAPP score is an easily applicable score that can be used by surgeons to evaluate the appendix during diagnostic laparoscopy. The score has high positive and negative predictive value. The LAPP score needs to be validated in a multicentre validation study.



Similar content being viewed by others


References
Bijnen CL, van den Broek WT, Bijnen AB et al (2003) Implications of removing a normal appendix. Dig Surg 20:215–219
Bakker OJ, Go PM, Puylaert JB, Kazemier G, Heij HA (2010) Guideline on diagnosis and treatment of acute appendicitis: imaging prior to appendectomy is recommended. Werkgroep richtlijn Diagnostiek en behandeling van acute appendicitis. Ned Tijdschr Geneeskd 154:A303
Andersson RE, Hugander A, Thulin AJ (1992) Diagnostic accuracy and perforation rate in appendicitis: association with age and sex of the patient and with appendicectomy rate. Eur J Surg 158:37–41
Marudanayagam R, Williams GT, Rees BI (2006) Review of the pathological results of 2,660 appendicectomy specimens. J Gastroenterol 41:745–749
Rosai J (2004) Rosai and Ackerman’s surgical pathology. 9th edn. Mosby, Edinburgh
Sauerland S, Agresta F, Bergamschi R et al (2006) Laparoscopy for abdominal emergencies. Surg Endosc 20:14–29
Korndorffer JR Jr, Fellinger E, Reed W (2010) SAGES guideline for laparoscopic appendectomy. Surg Endosc 24:757–761
van den Broek WT, Bijnen AB, de Ruiter P et al (2001) A normal appendix found during diagnostic laparoscopy should not be removed. Br J Surg 88:251–254
Flum DR, Koepsell T (2002) The clinical and economic correlates of misdiagnosed appendicitis: nationwide analysis. Arch Surg 137:799–804; discussion 804
van Dalen R, Bagshaw PF, Dobbs BR et al (2003) The utility of laparoscopy in the diagnosis of acute appendicitis in women of reproductive age. Surg Endosc 17:1311–1313
Moberg AC, Ahlberg G, Leijonmarck CE (1998) Diagnostic laparoscopy in 1,043 patients with suspected acute appendicitis. Eur J Surg 164:833–840
Teh SH, O’Ceallaigh S, McKeon JG et al (2000) Should an appendix that looks “normal” be removed at diagnostic laparoscopy for acute right iliac fossa pain? Eur J Surg 166:388–389
Kraemer M, Ohmann C, Leppert R et al (2000) Macroscopic assessment of the appendix at diagnostic laparoscopy is reliable. Surg Endosc 14:625–633
Kaselas C, Molinaro F, Lacreuse I et al (2009) Postoperative bowel obstruction after laparoscopic and open appendectomy in children: a 15-year experience. J Pediatr Surg 44:1581–1585
Leun TT, Dixon E, Gill M (2009) Bowel obstruction following appendectomy: what is the true incidence? Ann Surg 250:51–53
Andersson RE (2001) Small bowel obstruction after appendectomy. Br J Surg 88:1387–1391
Alvarado A (1986) A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med 15:557–564
Coursey CA, Nelson RC, Patel MB et al (2010) Making the diagnosis of acute appendicitis: do more preoperative CT scans mean fewer negative appendectomies? A 10-year study. Radiology 254:460–468
Pickhardt PJ, Lawrence EM, Pooler BD et al (2011) Diagnostic performance of multidetector computed tomography for suspected acute appendicitis. Ann Intern Med 154:789–796
Collaborative SCOAP, Cuschieri J, Florence M, Flum DR et al (2008) Negative appendectomy and imaging accuracy in the Washington State Surgical Care and Outcomes Assessment Program. Ann Surg 248:557–563
Wagner PL, Eachempati SR, Soe K et al (2008) Defining the current negative appendectomy rate: For whom is preoperative computed tomography making an impact? Surgery 144:276–282
Kim K, Kim YH, Kim SY et al (2012) Low dose abdominal CT for evaluating suspected appendicitis. N Engl J Med 366:1596–1605
Disclosures
Authors Jenneke T. H. Hamminga, H. Sijbrand Hofker, Paul M. A. Broens, Philip M. Kluin, Erik Heineman and Jan Willem Haveman have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
The study was conducted for the Apple Study Group; Appendicitis and Laparoscopic evaluation.
Rights and permissions
About this article
Cite this article
Hamminga, J.T.H., Hofker, H.S., Broens, P.M.A. et al. Evaluation of the appendix during diagnostic laparoscopy, the laparoscopic appendicitis score: a pilot study. Surg Endosc 27, 1594–1600 (2013). https://doi.org/10.1007/s00464-012-2634-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-012-2634-4