
Abstract
Background
To assess the diagnostic effectiveness, cardiopulmonary safety, and patient comfort of transnasal endoscopy (TNE), compared with conventional endoscopy (CES) and sedated endoscopy (SES), and to compare procedural risks and patient satisfaction/preference.
Methods
In this prospective, randomized, and controlled protocol, eligible patients (n = 397) in an outpatient clinic were randomized to CES (n = 133), SES (n = 134), or unsedated TNE (n = 130) due to upper gastrointestinal (GI) complaints. Patients were continuously monitored for systolic/diastolic blood pressure (SBP/DBP), pulse rate (PR), and SpO2 throughout the endoscopy. All subjects (n = 392) completing their assigned endoscopy were asked to evaluate endoscopy satisfaction, pain, and nausea/vomiting on visual analog scales. Patient preference for the assigned endoscopy was assessed against previous endoscopy experience or by willingness to repeat the assigned endoscopy.
Results
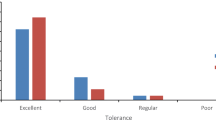
Endoscopic outcomes for the esophagus, stomach, and duodenum were comparable among the three groups. SBP/DBP and PR were more stable in patients undergoing TNE than in those undergoing CES or SES, while SpO2 remained stable and above 95 % among all three groups. Patients were more satisfied with TNE than with CES and experienced less pain and nausea/vomiting. Patients exhibited a high preference for SES, whereas 67.6 % of patients who previously underwent SES and were randomly assigned to TNE were willing to undergo TNE again.
Conclusions
TNE has comparable diagnostic effectiveness to CES and SES, but is less stressful on cardiopulmonary function, indicating that TNE is a more comfortable, preferred, and cost-effective endoscopic technique than CES and SES.




Similar content being viewed by others


References
Carey EJ, Sorbi D (2004) Unsedated endoscopy. Gastrointest Endosc Clin N Am 14:369–383
Eisen GM, Baron TH, Dominitz JA, Faigel DO, Goldstein JL, Johanson JF, Mallery JS, Raddawi HM, Vargo JJ II, Waring JP, Fanelli RD, Wheeler-Harbough J, American Society for Gastrointestinal Endoscopy (2002) Complications of upper GI endoscopy. Gastrointest Endosc 55:784–793
Iqbal CW, Askegard-Giesmann JR, Pham TH, Ishitani MB, Moir CR (2008) Pediatric endoscopic injuries: incidence, management, and outcomes. J Pediatr Surg 43:911–915
Meining A, Semmler V, Kassem AM, Sander R, Frankenberger U, Burzin M, Reichenberger J, Bajbouj M, Prinz C, Schmid RM (2007) The effect of sedation on the quality of upper gastrointestinal endoscopy: an investigator-blinded, randomized study comparing propofol with midazolam. Endoscopy 39:345–349
Cohen LB (2008) Patient monitoring during gastrointestinal endoscopy: why, when, and how? Gastrointest Endosc Clin N Am 18:651–663
Abraham N, Barkun A, Larocque M, Fallone C, Mayrand S, Baffis V, Cohen A, Daly D, Daoud H, Joseph L (2002) Predicting which patients can undergo upper endoscopy comfortably without conscious sedation. Gastrointest Endosc 56:180–189
Douma KF, Bleiker EM, Aaronson NK, Cats A, Gerritsma MA, Gundy CM, Vasen HF (2010) Long-term compliance with endoscopic surveillance for familial adenomatous polyposis. Colorectal Dis 12:1198–1207
Feld AD (2008) Endoscopic sedation: medicolegal considerations. Gastrointest Endosc Clin N Am 18:783–788
Hazeldine S, Fritschi L, Forbes G (2010) Predicting patient tolerance of endoscopy with conscious sedation. Scand J Gastroenterol 45:1248–1254
Abraham NS, Fallone CA, Mayrand S, Huang J, Wieczorek P, Barkun AN (2004) Sedation versus no sedation in the performance of diagnostic upper gastrointestinal endoscopy: a Canadian randomized controlled cost-outcome study. Am J Gastroenterol 99:1692–1699
Akyuz U, Pata C, Senkal V, Erzin Y (2010) Is propofol sedation with midazolam induction safe during endoscopic procedures without anesthesiologist? Hepatogastroenterology 57:685–687
Riphaus A, Lechowicz I, Frenz MB, Wehrmann T (2009) Propofol sedation for upper gastrointestinal endoscopy in patients with liver cirrhosis as an alternative to midazolam to avoid acute deterioration of minimal encephalopathy: a randomized, controlled study. Scand J Gastroenterol 44:1244–1251
Kerker A, Hardt C, Schlief HE, Dumoulin FL (2010) Combined sedation with midazolam/propofol for gastrointestinal endoscopy in elderly patients. BMC Gastroenterol 10:11
Stroppa I, Grasso E, Paoluzi OA, Razzini C, Tosti C, Andrei F, Biancone L, Palmieri G, Romeo F, Pallone F (2008) Unsedated transnasal versus transoral sedated upper gastrointestinal endoscopy: a one-series prospective study on safety and patient acceptability. Dig Liver Dis 40:767–775
Yuki M, Amano Y, Komazawa Y, Fukuhara H, Shizuku T, Yamamoto S, Kinoshita Y (2009) Unsedated transnasal small-caliber esophagogastroduodenoscopy in elderly and bedridden patients. World J Gastroenterol 15:5586–5591
Dean R, Dua K, Massey B, Berger W, Hogan WJ, Shaker R (1996) A comparative study of unsedated transnasal esophagogastroduodenoscopy and conventional EGD. Gastrointest Endosc 44:422–424
Yagi J, Adachi K, Arima N, Tanaka S, Ose T, Azumi T, Sasaki H, Sato M, Kinoshita Y (2005) A prospective randomized comparative study on the safety and tolerability of transnasal esophagogastroduodenoscopy. Endoscopy 37:1226–1231
Mori A, Ohashi N, Tatebe H, Maruyama T, Inoue H, Takegoshi S, Kato T, Okuno M (2008) Autonomic nervous function in upper gastrointestinal endoscopy: a prospective randomized comparison between transnasal and oral procedures. J Gastroenterol 43:38–44
Kim CY, O’Rourke RW, Chang EY, Jobe BA (2006) Unsedated small-caliber upper endoscopy: an emerging diagnostic and therapeutic technology. Surg Innov 13:31–39
Horiuchi A, Nakayama Y, Hidaka N, Ichise Y, Kajiyama M, Tanaka N (2009) Prospective comparison between sedated high-definition oral and unsedated ultrathin transnasal esophagogastroduodenoscopy in the same subjects: pilot study. Dig Endosc 21:24–28
Dumortier J, Josso C, Roman S, Fumex F, Lepilliez V, Prost B, Lot M, Guillaud O, Petit-Laurent F, Lapalus MG, Ponchon T (2007) Prospective evaluation of a new ultrathin one-plane bending videoendoscope for transnasal EGD: a comparative study on performance and tolerance. Gastrointest Endosc 66:13–19
Tatsumi Y, Harada A, Matsumoto T, Tani T, Nishida H (2009) Current status and evaluation of transnasal esophagogastroduodenoscopy. Dig Endosc 21:141–146
Cho S, Arya N, Swan K, Cirocco M, Kandel G, Kortan P, Marcon N (2008) Unsedated transnasal endoscopy: a Canadian experience in daily practice. Can J Gastroenterol. 22(3):243–246
Murata A, Akahoshi K, Sumida Y, Yamamoto H, Nakamura K, Nawata H (2007) Prospective randomized trial of transnasal versus peroral endoscopy using an ultrathin videoendoscope in unsedated patients. J Gastroenterol Hepatol 22:482–485
Dua KS, Ruan E, Shaker R (1996) Transnasal pharyngoesophagogastroduodenoscopy (T-PEGD) in a patient with acute upper gastrointestinal bleeding. Endoscopy 28:530
Disclosures
Zheng-Lin Ai, Chun-Hui Lan, Li-Lin Fan, Li Lan, Yan Cao, Ping Li, Ou Song, Dong-Feng Chen have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ai, ZL., Lan, CH., Fan, LL. et al. Unsedated transnasal upper gastrointestinal endoscopy has favorable diagnostic effectiveness, cardiopulmonary safety, and patient satisfaction compared with conventional or sedated endoscopy. Surg Endosc 26, 3565–3572 (2012). https://doi.org/10.1007/s00464-012-2367-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-012-2367-4