
Abstract
Background
Recent studies document excess weight loss (EWL) of more than 50% with the laparoscopic adjustable gastric band (LGB). This study reviews the LGB experience at an urban academic center in terms of complications, reoperative rates, and comorbidities.
Methods
In this study, 144 consecutive patients undergoing LGB were prospectively reviewed. Data were collected including weight, body mass index (BMI), excess weight loss (EWL), comorbidities, and complications. Demographics were analyzed using a t-test. Linear regression was used to analyze the relationship of BMI, race, and age to EWL at 12 months.
Results
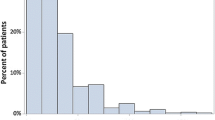
The study participants were 130 women with a mean age of 43 ± 11 years, a mean weight of 127.1 kg ± 20.5 kg, and a mean BMI of 45.6 ± 6.1. The mean follow-up period was 16 months. The mean EWL was 20% ± 14% at 6 months (n = 118), 26% ± 16% at 12 months (n = 106), 30% ± 20% at 18 months (n = 68), and 34% ± 23% at 24 months (n = 43). Patients with a BMI higher than 50 kg/m2 had a lower EWL at 12 months than patients with a BMI lower than 50 kg/m2 (P = 0.00005). The mean EWL at 12 months was significantly less for African Americans than for Caucasians (P = 0.0046; 95% confidence interval [CI] 3–15%). Patients older than 50 years had a lower EWL, but the difference was not statistically significant (P = 0.07). Complete and partial resolution of comorbidities occurred for 10% and 4% of the patients, respectively. Removal of the band with revision to a sleeve gastrectomy for inadequate EWL was required for 14 patients (11.5%). Complications occurred for 8% of the patients (n = 15) including port flipping, stoma obstruction, tube disconnection, port infections, dysphagia, and band slippage. Overall, 16.7% of the patients (n = 24) required reoperation.
Conclusion
After LGB, a majority of the patients failed to achieve a 50% EWL, and 16.7% required reoperation. Laparoscopic adjustable gastric banding may not be the optimal bariatric procedure for patients older than 50 years, patients with a BMI higher than 50 kg/m2, or African Americans.


Similar content being viewed by others


References
Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM (2006) Prevalence of overweight and obesity in the United States, 1999–2004. JAMA 295:1549–1555
Cristou NV, Sampalis JS, Libermann M, Look D, Auger S, McLean AP, MacLean LD (2004) Surgery decreases long-term mortality, morbidity, and health care use in morbidly obese patients. Ann Surg 240:416–424
Peeters A, O’Brien PE, Laurie C, Anderson M, Wolfe R, Flum D, MacInnis RJ, English DR, Dixon J (2007) Substantial intentional weight loss and mortality in the Severely Obese. Ann Surg 246:1028–1033
O’brien P, Dixon JB, Laurie C, Skinner S, Proietto J, McNeil J, Strauss B, Marks S, Schachter L, Chapman L, Anderson M (2006) Treatment of mild to moderate obesity with laparoscopic adjustable gastric banding or an intensive medical program. Ann Int Med 144:625–633
Gagner M, Milone L, Yung E, Broseus A, Gumbs A (2008) Causes of early mortality after laparoscopic adjustable gastric banding. J Am Coll Surg 206:664–669
Martin LF, Smits GJ, Greenstein RJ (2007) Treating morbid obesity with laparoscopic adjustable gastric banding. Am J Surg 194:333–343
Parikh MS, Fielding GA, Ren CJ (2005) U.S. experience with 749 laparoscopic adjustable gastric bands: intermediate outcomes. Surg Endosc 19:1631–1635
R Development Core Team (2006) R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. ISBN 3-900051-07-0, http://www.R-project.org. Accessed 1 May 2009
Galvani C, Gorodner M, Moser F, Baptista M, Chretien C, Berger R, Horgan S (2006) Laparoscopic adjustable gastric band versus laparoscopic Roux-en Y gastric bypass: ends justify the means? Surg Endosc 20:934–941
Chapman AE, Kiroff G, Game P, Foster B, O’Brien P, Ham J, Maddern GJ (2004) Laparoscopic adjustable gastric banding in the treatment of obesity: a systematic literature review. Surgery 135:326–351
DeMaria E, Sugarman H, Meador J, Doty J, Kellum J (2001) High failure rate after laparoscopic adjustable silicone gastric banding for treatment of morbid obesity. Ann Surg 233:809–818
Doherty C, Maher J, Heitshusen D (2002) Long-term data indicate a progressive loss in efficacy of adjustable silicone gastric banding for the surgical treatment of morbid obesity. Surgery 132:724–728
Ceelen W, Walder J, Cardon A, Renteghem KV, Hesse U, Malt ME, Pattyn P (2003) Surgical treatment of severe obesity with a low pressure adjustable gastric band. Ann Surg 237:10–16
Angrisani L, Furbetta F, Doldi SB, Basso N, Lucchese M (2003) LapBand adjustable gastric banding system: the Italian experience with 1,863 patients operated on 6 years. Surg Endosc 17:409–412
Zehetner J, Holzinger F, Triaca H, Ch Klaiber (2005) A 6-year experience with the Swedish adjustable gastric band. Surg Endosc 19:21–28
Anwar M, Collins J, Kow L, Toouli J (2008) Long-term efficacy of a low-pressure adjustable gastric band in the treatment of morbid obesity. Ann Surg 247:771–778
Allen J (2007) Laparoscopic gastric band complications. Med Clin North Am 91:485–497
Spivak H, Favretti F (2002) Avoiding postoperative complications with the LAP-BAND system. Am J Surg 184:31S–37S
Chouselb E, Szomstein S, Lomenzo E, Higa G, Podkameni D, Soto F, Zundel N, Rosenthal R (2005) Laparoscopic removal of gastric band after early gastric erosion. Surg Laparosc Endosc Percutan Tech 15:24–27
Nocca D, Frering V, Gallix B, des Hons C, Noël P, Foulonge MA, Millat B, Fabre JM (2005) Migration of adjustable gastric banding froma cohort study of 4,236 patients. Surg Endosc 19:947–950
Biertho L, Steffen R, Branson R, Potoxzna N, Ricklin T, Piec G, Horber FF (2004) Management of failed adjustable gastric banding. Surgery 137:33–41
Müller MK, Attigah N, Wildi S, Hahnloser D (2008) High secondary failure rate of rebanding after failed gastric banding. Surg Endosc 22:448–453
Edwards MA, Grinbaum R, Schneider BE, Walsh A, Ellsmere J, Jones DB (2007) Benchmarking hospital outcomes for laparoscopic adjustable banding. Surg Endosc 21:1950–1956
Disclosures
Jason Kasza, Fred Brody, Khashayar Vaziri, Carl Scheffey, Sheldon Mcmullan, Brian Wallace, and Fatima Khambaty have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kasza, J., Brody, F., Vaziri, K. et al. Analysis of poor outcomes after laparoscopic adjustable gastric banding. Surg Endosc 25, 41–47 (2011). https://doi.org/10.1007/s00464-010-1126-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-010-1126-7