
Abstract
Background
A majority of abdominal injuries (AIs) are associated with shock, hence most of the patients are hemodynamically unstable, which limits the use of video-assisted laparoscopy (VAL) in their management. The purpose of this study is to demonstrate the possibility of using VAL in management of stable and unstable patients with abdominal trauma.
Methods
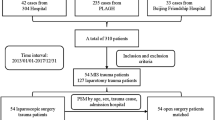
In a period of six years 2,695 patients with AIs were evaluated. The subjects were evaluated retrospectively and divided into two groups. Group 1, consisting of 1,363 patients, had conventional routine investigations following which they underwent laparotomy for confirmatory diagnosis and definitive management. The second group, consisting of 1,332 patients, underwent diagnostic laparoscopy in addition to the conventional investigations in the first group; 411 patients of this group had therapeutic laparoscopy.
Demographic information, incidence of organs injuries and operative findings, success rate of VAL and laparotomy repair, complications, associated injuries, and hospital mortality were evaluated.
Results
The age of 62.6% of our patients was 20–50 years, while 10.6% and 14.5% were less than 19 and greater than 50 years, respectively. Associated injuries were head, chest, musculoskeletal, and vertebral column. Most of the victims presented with shock; 50.7%, 24.7%, and 15.9% of the patients were in mild, moderate, and severe shock respectively, and 8.7% of the subjects had stable hemodynamic status. In the first group 47.1% of the laparotomies were absolutely indicated and 24.4% were negative. Of the patients who had laparotomy, 26.0% would have been managed confidently by VAL. In the second group following VAL 42.5% of the patients did not require surgical intervention. VAL surgery was performed in 30.8% of patients. Conversion to laparotomy was performed in 26.7% of the patients.
Conclusions
The VAL technique can be confidently used as a main tool to expedite evaluation and treatment of patients with abdominal trauma in cases of both stable and unstable hemodynamic status.
Similar content being viewed by others


References
Carey JE, Koo R, Miller R, Stein M (1995) Laparoscopy and thoracoscopy in evaluation abdominal trauma. Am Surg 61:92–95
Demetriades D, Velmahos G (2003) Technology-driven triage of abdominal trauma. The emerging era of nonoperative management. Annu Rev Med 54:1–15
Friese R, Coln C, Gentilello L (2005) Laparoscopy is sufficient to exclude occult diaphragm injury after penetrating abdominal trauma. J Trauma 58:789–792
Jason S, Erica C, Scott D, Bin J, Michael S (2005) Abdominal trauma: a disease in evolution. ANZ J Surg 75:790–810
Juan A, Hector A, William V, Walter W, Esteban G, Gustavo A, James M, George V, Demetrios D (2002) Penetrating thoracoabdominal injuries: ongoing dilemma-which cavity and when? World J Surg 26:539–543
Lawrence W, Gerard M (2003) Management of injured patients. In: James R, William C, Frank R (eds) Current surgical diagnosis and treatment. Lange, New York, pp. 230–255
Lujan A, Parrilla P, Robles R, Torralba J, Sanchez F, Arenas J (1995) Laparoscopic surgery in the management of traumatic hemoperitoneum in stable patients. Surg Endosc 9:879–881
Martinez M, Briz J, Carillo1 E (2001) Video thoracoscopy expedites the diagnosis and treatment of penetrating diaphragmatic injuries. Surg Endosc 15:28–32
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cherkasov, M., Sitnikov, V., Sarkisyan, B. et al. Laparoscopy versus laparotomy in management of abdominal trauma. Surg Endosc 22, 228–231 (2008). https://doi.org/10.1007/s00464-007-9550-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-007-9550-z