
Abstract
Background
The vertical gastrectomy (VG) is the restrictive part of the technically difficult biliopancreatic diversion with duodenal switch operation (DS). The VG was originally conceived of as an independent operation—the first stage of a two-stage DS that would reduce mortality and morbidity in the high-risk superobese because of a shorter operating time and no anastomoses. This article presents two-year data after VG.
Methods
Laparoscopic VG was performed in a nonrandomized fashion in obese patients that met the NIH criteria for bariatric surgery. By using 5–7 firings of 45–60-mm linear 3.5-mm GI staplers along a 32-Fr bougie, a greater-curvature gastrectomy is performed and a 60–80-ml gastric tube is created. VG was compared to adjustable Lap-Band® placement, Roux-en-Y gastric bypass (RGB), and DS.
Results
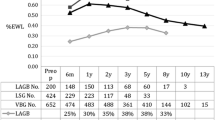
Between November 2002 and August 2005, 216 patients underwent VG. The mean age was 44.7 years (range = 16–64) and 173 (80%) were female. The mean preoperative weight and body mass index (BMI) was 302 ± 77 lbs and 49 ± 11 kg/m2, respectively. Of the 216 patients, 5 (2.3%) had a BMI > 80 kg/m2, 6 (2.8%) had a BMI of 70–80 kg/m2, and 25 (11.6%) had a BMI of 60–70 kg/m2. The mean operative time was 66 ± 11 min (range = 45–180) and the mean length of hospital stay was 1.9 ± 1.2 days. Complications occurred in 20 (6.3%) patients (vs. 7.1% after Lap-Band). Leaks occurred in 3 (1.4%) VG patients, reoperations were performed in 6 (2.8%), and no conversions to open or deaths occurred. Weight loss on par with the DS and RGB was achieved with just the VG alone.
Conclusion
The VG operation is able to achieve significant weight loss comparable to the RGB and DS operations but with the low morbidity profile similar to that of Lap-Band placement.




Similar content being viewed by others


Abbreviations
- Band:
-
adjustable gastric band placement
- BMI:
-
body mass index
- DS:
-
Hess’ biliopancreatic diversion and duodenal switch (also known as the vertical gastrectomy and duodenal switch)
- EBL:
-
estimated blood loss
- %EWL:
-
percentage excess weight loss
- ICU:
-
intensive care unit
- POD:
-
postoperative day
- RGB:
-
Roux-en-Y gastric bypass
- VBG:
-
vertical banded gastroplasty
- VG:
-
vertical gastrectomy
References
Baltasar A, Bou R, Bengochea M, Arlandis F, Escriva C, Miro J, Martinez R, Perez N (2001) Duodenal Switch: an effective therapy for morbid obesity—intermediate results. Obes Surg 11: 54–58
Camerini G, Adami G, Marinari GM, Gianetta E, Pretolesi F, Papadia F, Marini P, Murelli F, Carlini F, Stabilini C, Sormani MP, Scopinaro N (2004) Thirteen years of follow-up in patients with adjustable silicone gastric banding for obesity: weight loss and constant rate of late specific complications. Obes Surg 14: 1343–1348
Fielding GA, Allen JW (2002) A step-by-step guide to placement of the LAP-BAND adjustable gastric banding system. Am J Surg 184(6B): 26S–30S
Hess DS, Hess DW (1998) Biliopancreatic diversion with a duodenal switch. Obes Surg 8(3): 267–282
Higa KD, Boone KB, Ho T, Davies OG (2000) Laparoscopic Roux-en-Y gastric bypass for morbid obesity: technique and preliminary results of our first 400 patients. Arch Surg 135(9): 1029–1033
Johnston D, Dachtler J, Sue-Ling HM, King RF, Martin G (2003) The Magenstrasse and Mill operation for morbid obesity. Obes Surg 13: 10–16
Kim WW, Gagner M, Kini S, Inabnet WB, Quinn T, Herron D, Pomp A (2003) Laparoscopic vs. open biliopancreatic diversion with duodenal switch: a comparative study. J Gastrointest Surg 7(4): 552–557
Marceau P, Hould FS, Simard S, Lebel S, Bourque RA, Potvin M, Biron S (1998) Biliopancreatic diversion with duodenal switch. World J Surg 22(9): 947–954
Mason EE (1982) Vertical banded gastroplasty for morbid obesity. Arch Surg 117: 701–706
Olbers T, Lonrith H, Dalenback J, Haglind E, Lundell L (2001) Laparoscopic vertical banded gastroplasty – an effective long-term therapy for morbidly obese patients? Obes Surg 11(6): 726–730
Perez N, Baltasar A, Serra C, Ferri L, Bou R, Bengochea M (2005) Comparative analysis of vertical banded gastroplasty and duodenal switch at five years follow-up. Obes Surg 15(7): 1061–1065
Printen KJ, Mason EE (1973) Gastric surgery for relief of morbid obesity. Arch Surg 106: 428–431
Author information
Authors and Affiliations
Corresponding author
Additional information
Presented at the Plenary Session of the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES), Dallas, TX, 28 April 2006
Rights and permissions
About this article
Cite this article
Lee, C.M., Cirangle, P.T. & Jossart, G.H. Vertical gastrectomy for morbid obesity in 216 patients: report of two-year results. Surg Endosc 21, 1810–1816 (2007). https://doi.org/10.1007/s00464-007-9276-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-007-9276-y