
Abstract
Background
Bevacizumab is frequently combined with 5-fluorouracil-based chemotherapy for patients with metastatic colorectal cancer (mCRC). The relative benefit of bevacizumab in older patients has not been widely studied and is of interest.
Patients and methods
This retrospective analysis used data from three first-line randomized controlled studies and one second-line randomized controlled study of bevacizumab plus chemotherapy in medically fit (Eastern Cooperative Oncology Group performance status 0 or 1) patients with mCRC. Overall survival (OS) and on-treatment progression-free survival (PFS) were assessed in patients aged <65, ≥65, and ≥70 years. Results were compared using unstratified hazard ratios (HRs). Grade 3–5 adverse events were also assessed.
Results
Bevacizumab statistically significantly improved PFS [HR 0.58; 95% confidence interval (CI) 0.49–0.68] and OS (HR 0.85; 95% CI 0.74–0.97) in patients aged ≥65 years; patients aged ≥70 years had similar improvements. Benefits were consistent across the studies, irrespective of setting, bevacizumab dose, or chemotherapy regimen. Increases in thromboembolic events were observed in patients aged ≥65 and ≥70 years in the bevacizumab group compared with the control group, mainly as a result of increases in arterial thromboembolic events. No other substantial age-related increases in grade 3–5 adverse events were observed.
Conclusions
In medically fit older patients, bevacizumab provides similar PFS and OS benefits as in younger patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Two-thirds of patients newly diagnosed with metastatic colorectal cancer (mCRC) are aged ≥65 years and 40% of cases occur in patients aged ≥75 years (Edwards et al. 2002). Older patients represent a heterogeneous population, and chemotherapy in these individuals must be considered alongside declining end organ function and physical and psychological conditions that can compromise the effective administration of chemotherapy. Many clinical trials therefore exclude older patients, particularly those with poor performance status, and few age-specific studies have been published. Even in trials with no upper age limit, the proportion of older and very old patients is usually small, probably reflecting the more conservative approach adopted by clinicians when treating these patients. Consequently, fewer older patients are eligible for clinical trials and reliable evidence supporting the benefits of chemotherapy in this population is limited.
To overcome the underrepresentation of older patients in clinical trials, pooled analyses have been performed to investigate the efficacy and tolerability of treatment in more meaningful numbers of patients. Previous analyses have indicated that chemotherapy with 5-fluorouracil (5-FU), 5-FU/oxaliplatin, or 5-FU/irinotecan is feasible for selected older patients with mCRC (Folprecht et al. 2004, 2008; Goldberg et al. 2006). Folprecht and colleagues (2008) reported that patients aged ≥70 years did not generally experience greater toxicity than younger patients, although hepatotoxicity was more common in older patients. These analyses provide a strong rationale for the treatment of suitable older patients with effective chemotherapy.
Bevacizumab is commonly used with chemotherapy in the treatment of patients with mCRC. Most patients included in bevacizumab clinical trials have been <65 years old, and thus its efficacy and tolerability in older patients are less well established. A previous pooled analysis examined the efficacy and safety of bevacizumab in 438 patients (Kabbinavar et al. 2009). Since that analysis was undertaken, the results of larger, randomized, placebo-controlled studies have become available, thus expanding the number of older patients for whom efficacy and safety data are available. The present retrospective analysis was therefore undertaken to compare the efficacy and safety of bevacizumab plus chemotherapy in older versus younger patients with mCRC who participated in four randomized phase II and III trials that included over 1,100 patients aged ≥65 years.
Patients and methods
Study design
This analysis included data from three first-line [AVF2107g (Hurwitz et al. 2004); AVF2192g (Kabbinavar et al. 2005); NO16966 (Saltz et al. 2008)] and one second-line [E3200 (Giantonio et al. 2007)] multicenter randomized trials. Patients were treated with fluoropyrimidine-based chemotherapy with or without bevacizumab. Only the principal arms in these studies were included in the current analysis. In study NO16966, patients were treated with first-line oxaliplatin + 5-FU/leucovorin (LV) (FOLFOX4) or capecitabine (XELOX) ± bevacizumab (Saltz et al. 2008). Patients in AVF2107g were initially randomized to 5-FU/LV + bevacizumab, 5-FU/LV + irinotecan (IFL) + placebo, or IFL + bevacizumab, although recruitment to the 5-FU/LV plus bevacizumab arm was halted after an interim analysis (Hurwitz et al. 2004). Patients in AVF2192g were randomized to 5-FU/LV + placebo or bevacizumab (Kabbinavar et al. 2005) and patients in study E3200, who had failed previous fluoropyrimidine–irinotecan therapy, were randomized to FOLFOX4 ± bevacizumab (Giantonio et al. 2007).
Assessments
Overall survival (OS) and on-treatment progression-free survival (PFS)—common endpoints in all four trials—were evaluated in patients <65 years, ≥65 years, and ≥70 years in each study and as a pooled analysis. Intention to treat PFS was not evaluated in all of the four studies. On-treatment PFS was a secondary endpoint in all four trials; OS was the primary endpoint in AVF2107g, AVF2192g, and E3200 and a secondary endpoint in NO16966.
Definitions of on-treatment PFS varied by study. In NO16966, patients were censored for curative surgery but not for other second-line treatment. On-treatment analysis included tumor assessments and death occurring ≤28 days after the last study medication intake during the primary treatment phase. Patients without an event during this phase were censored at the last tumor assessment date or on day 1 if no post-baseline assessment was available. Patients with curative-intent surgical resection without prior progression ≤28 days after the last study medication intake in the primary phase were censored at the surgery date. In AVF2107g and AVF2192g, on-treatment PFS was defined as the time from randomization to disease progression or death from any cause during first-line therapy (deaths ≤30 days after the last study drug dose during first-line treatment were considered as events). In E3200, clinical deterioration was not considered an event; censoring was performed for second-line treatment. PFS was defined as the time from randomization to disease progression or any-cause death ≤30 days after study treatment discontinuation. Data for patients without disease progression or death at the time of analysis were censored at the last tumor assessment ≤30 days after the last dose (or, if no post-baseline tumor assessments were performed, at the time of randomization plus 1 day). Data for patients who discontinued any treatment component or received nonprotocol-specified therapy before disease progression were censored at the time of the last tumor assessment during treatment.
Adverse events of interest for bevacizumab were assessed by age group. Data collection varied among trials; only grade 3–5 data were collected consistently in the studies and only these events were pooled for the current analysis.
Statistical analyses
Efficacy analysis was based on all randomized patients (intent-to-treat analysis). The primary outcome was OS, defined as time from randomization to death. PFS, defined as time from randomization to disease progression or death from any cause during first-line treatment, was a secondary outcome.
Integrated analyses were stratified by study. Unstratified hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated for each study to allow comparisons. Results therefore differ slightly from the primary analyses of each study report: for example, the primary analysis of NO16966 used a 97.5% CI and was stratified by chemotherapy treatment (Saltz et al. 2008). The unstratified point estimate (HR) for NO16966, however, remains the same as that in the study report. Similarly, for the other three studies, the results shown are for the unstratified analysis, i.e. not stratifying according to the stratification variables used at randomization. Kaplan–Meier methods were used to estimate median OS and on-treatment PFS durations. Durations of OS and on-treatment PFS in the pooled bevacizumab group and the pooled control group were compared using two-sided stratified log-rank tests.
Results
In total, 3,007 patients were eligible for inclusion in the analysis; 1,864 were aged <65 years (914, 542, 41, and 367 patients in studies NO16966, AVF2107g, AVF2192g, and E3200, respectively), 1,142 were ≥65 years (486, 271, 168, and 217 patients, respectively), 712 patients were ≥70 years (268, 176, 138, and 130 patients, respectively), and the age of one patient was unknown. Patient baseline characteristics were generally well balanced between the age groups (Table 1). A general worsening of Eastern Cooperative Oncology Group performance status (ECOG PS) was observed with age.
Efficacy of bevacizumab by age group
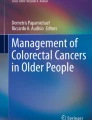
Addition of bevacizumab to chemotherapy significantly prolonged PFS in older and younger patients (Fig. 1a–c). The magnitude of PFS benefit was similar in both older (aged ≥65 years and ≥70 years) and younger patients. In patients aged <65 years, median PFS was 9.5 months for bevacizumab versus 6.7 months for the control (P < 0.0001); in those aged ≥65 years, median PFS was 9.3 months for bevacizumab versus 6.9 months for the control (P < 0.0001); and in those aged ≥70 years, median PFS was 9.2 months for bevacizumab versus 6.4 months for the control (P < 0.0001). HRs are shown in Table 2. Point estimates were consistent across the trials, indicating a similar treatment effect irrespective of setting (first or second line), bevacizumab dose (2.5 mg/kg/week or 5 mg/kg/week), chemotherapy regimen (5-FU/LV, IFL, XELOX, or FOLFOX4), or age.

Progression-free survival and overall survival stratified by age across randomized trials in patients with metastatic colorectal cancer. Progression-free survival in patients aged a <65 years, b ≥65 years, and c ≥70 years; overall survival in patients aged d <65 years, e ≥65 years, and f ≥70 years
Adding bevacizumab to chemotherapy statistically significantly prolonged OS in both older and younger patients (Table 2; Fig. 1d–f), although the magnitude of effect was smaller than for PFS. When OS data from the individual studies were analyzed by age, results for the age groups were generally similar to the overall study data. In patients aged <65 years, median OS was 19.9 months for bevacizumab versus 16.5 months for the control (P < 0.0001); in those aged ≥65 years, median OS was 17.9 months for bevacizumab versus 15.0 months for the control (P = 0.015); and in those aged ≥70 years, median OS was 17.4 months for bevacizumab versus 14.1 months for the control (P = 0.005).
Safety of bevacizumab by age group
Rates of adverse events of special interest with bevacizumab are shown in Fig. 2. Bleeding, hypertension, proteinuria, arterial thromboembolic events (ATEs), venous thromboembolic events (VTEs), wound-healing complications, fistulae, gastrointestinal perforation, and congestive heart failure were more common in bevacizumab-treated patients. ATEs and VTEs were more frequent in older versus younger patients in the control and bevacizumab groups. In patients aged <65 years, there was no difference in ATE rates in the bevacizumab and control groups (2% incidence in both groups). However, in patients aged ≥65 years, the ATE rate was 5.7% for bevacizumab patients versus 2.5% for the control group; in patients aged ≥70 years, the incidence of ATEs was 6.7% with bevacizumab versus 3.2% with control. In contrast, VTEs were consistently 1–2% more frequent with bevacizumab versus control, but did not appear to increase to a relatively greater degree with age. Gastrointestinal perforations occurred in 14 bevacizumab-treated patients (<1%; eight events in patients <65 years and six in patients ≥65 years, four of which occurred in patients aged ≥70 years) and two control patients (<1%; both aged <65 years).

Adverse events of interest for bevacizumab in randomized trials of patients with metastatic colorectal cancer. ATE arterial thromboembolic event, CHF congestive heart failure, GI gastrointestinal, VTE venous thromboembolic event, WHC wound-healing complication
Adverse events leading to death occurred in 17 bevacizumab-treated patients; seven were aged <65 years and 10 were aged ≥65 years. Eleven control group patients had adverse events leading to death; five were aged <65 years and six were aged ≥65 years. In patients aged ≥70 years, adverse events resulting in death occurred in six bevacizumab-treated patients and three control group patients.
Rates of on-study death from any cause appeared to be lower in bevacizumab-treated patients (<65 years 69 vs. 75%, ≥65 years 74 vs. 77%, ≥70 years 76 vs. 81%, for bevacizumab vs. control, respectively). The proportion of nontumor-related deaths increased with age, from 18% in patients aged <65 years (17% for bevacizumab vs. 19% for control) to 22% in those aged ≥65 years (23% for bevacizumab vs. 21% for control) and 25% in those aged ≥70 years (25% for bevacizumab vs. 22% for control).
Discussion
The most significant finding of this retrospective exploratory pooled analysis of trials comparing chemotherapy plus bevacizumab with chemotherapy alone in mCRC was that within this protocol-eligible population, older and younger patients appeared to achieve similar survival benefits from bevacizumab treatment. Improvements in PFS were comparable in patients aged <65 years, ≥65 years, and ≥70 years, with HRs of 0.59, 0.58, and 0.54, respectively. Patients also showed statistically significant prolongation of median PFS with the addition of bevacizumab to their treatment, with a similar magnitude of PFS improvement in younger and older patients. The effect of bevacizumab was consistent across age groups in each study. Although statistically significant, the effect of bevacizumab on OS in older patients was not so pronounced as its effect on PFS, reflected by HRs of 0.77, 0.85, and 0.79 for patients aged <65 years, ≥65 years, and ≥70 years, respectively. Several reasons are possible: older bevacizumab patients were more likely to be less fit, with 41% of patients aged <65 years, 49% aged ≥65 years, and 52% aged ≥70 years being ECOG PS 1. Also, older patients had more comorbidities, as indicated by a higher rate of noncancer-related deaths in both arms.
The risk–benefit profile of bevacizumab treatment in these medically fit, older patients did not substantially alter with age for most toxicities recorded. Hypertension, bleeding, and proteinuria were the most commonly reported side effects, as previously described (Hurwitz and Saini 2006). Toxicity rates were generally similar in older and younger patients, although thromboembolic events, which increase in frequency with advancing age (Silverstein et al. 1998; Abbott et al. 2003; Goldberg et al. 1989), were more common in older patients in both the bevacizumab and control groups. The present study corroborates earlier reports that the risk of bevacizumab-related ATEs increases with age (Scappaticci et al. 2007). There were more ATEs in older bevacizumab-treated patients compared with younger bevacizumab-treated patients and, while the incidence of ATEs in patients aged <65 years was essentially similar with or without bevacizumab, the incidence was higher in bevacizumab versus control patients aged ≥65 and ≥70 years. There was no apparent increase in VTE rates with advancing age, consistent with previous reports. Among older patients in the BRiTE registry, the incidence of thromboembolic events increased with age, although the increase was not statistically significant after adjustment for baseline ECOG PS and prior history of thromboembolic events (Kozloff et al. 2008). The incidence of other bevacizumab-related events was similar in younger and older patients in BRiTE.
The present analysis complements and expands upon the findings of the smaller pooled analysis of older patients by Kabbinavar and colleagues (2009), which reported a benefit of adding bevacizumab to chemotherapy in medically fit patients aged ≥65 years without an increased risk of adverse events. As well as including a larger number of patients, the present analysis has the added advantage of directly comparing older and younger patients in contrast to the earlier study, in which the group of older patients was compared with the total population, rather than the younger patients. Taken together, these analyses suggest that bevacizumab-treated older patients who meet eligibility requirements for clinical trials are not at increased risk of adverse events, other than ATEs, compared with those aged <65 years. The present analysis of older patients considered those aged ≥65 years, higher than the median age in the pooled population, and supplemented this with an analysis of those aged ≥70 years, which more closely reflects the general population of patients presenting with colorectal cancer. It should be emphasized that patients in the present analysis and in the other studies cited were clinical-trial eligible and may not be representative of a more general elderly population. Careful selection of patients and monitoring of treatment effects are required to optimize bevacizumab use in older patients.
In conclusion, this pooled analysis of data from phase II and III mCRC studies demonstrates that bevacizumab in combination with chemotherapy had a similar impact on PFS and OS in protocol-eligible older versus younger patients. Careful patient selection, however, remains important and should include an objective assessment of the patient’s physical and mental status.
References
Abbott RD, Curb JD, Rodriguez BL, Masaki KH, Popper JS, Ross GW, Petrovitch H (2003) Age-related changes in risk factor effects on the incidence of thromboembolic and hemorrhagic stroke. J Clin Epidemiol 56:479–486
Edwards BK, Howe HL, Ries LA, Thun MJ, Rosenberg HM, Yancik R, Wingo PA, Jemal A, Feigal EG (2002) Annual report to the nation on the status of cancer, 1973–1999, featuring implications of age and aging on U.S. cancer burden. Cancer 94:2766–2792
Folprecht G, Cunningham D, Ross P, Glimelius B, Di Costanzo F, Wils J, Scheithauer W, Rougier P, Aranda E, Hecker H, Köhne CH (2004) Efficacy of 5-fluorouracil-based chemotherapy in elderly patients with metastatic colorectal cancer: a pooled analysis of clinical trials. Ann Oncol 15:1330–1338
Folprecht G, Seymour MT, Saltz L, Douillard JY, Hecker H, Stephens RJ, Maughan TS, Van Cutsem E, Rougier P, Mitry E, Schubert U, Köhne CH (2008) Irinotecan/fluorouracil combination in first-line therapy of older and younger patients with metastatic colorectal cancer: combined analysis of 2,691 patients in randomized controlled trials. J Clin Oncol 26:1443–1451
Giantonio BJ, Catalano PJ, Meropol NJ, O’Dwyer PJ, Mitchell EP, Alberts SR, Schwartz MA, Benson AB 3rd, Eastern Cooperative Oncology Group Study E3200 (2007) Bevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previously treated metastatic colorectal cancer: results from the Eastern Cooperative Oncology Group Study E3200. J Clin Oncol 25:1539–1544
Goldberg RJ, Gore JM, Gurwitz JH, Alpert JS, Brady P, Strohsnitter W, Chen ZY, Dalen JE (1989) The impact of age on the incidence and prognosis of initial acute myocardial infarction: the Worcester Heart Attack Study. Am Heart J 117:543–549
Goldberg RM, Tabah-Fisch I, Bleiberg H, de Gramont A, Tournigand C, Andre T, Rothenberg ML, Green E, Sargent DJ (2006) Pooled analysis of safety and efficacy of oxaliplatin plus fluorouracil/leucovorin administered bimonthly in elderly patients with colorectal cancer. J Clin Oncol 24:4085–4091
Hurwitz H, Saini S (2006) Bevacizumab in the treatment of metastatic colorectal cancer: safety profile and management of adverse events. Semin Oncol 33(5 Suppl 10):S26–S34
Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J, Heim W, Berlin J, Baron A, Griffing S, Holmgren E, Ferrara N, Fyfe G, Rogers B, Ross R, Kabbinavar F (2004) Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 350:2335–2342
Kabbinavar FF, Hambleton J, Mass RD, Hurwitz HI, Bergsland E, Sarkar S (2005) Combined analysis of efficacy: the addition of bevacizumab to fluorouracil/leucovorin improves survival for patients with metastatic colorectal cancer. J Clin Oncol 23:3706–3712
Kabbinavar F, Hurwitz H, Yi J, Rosen O (2009) Addition of bevacizumab to fluorouracil-based first-line treatment of metastatic colorectal cancer: pooled analysis of cohorts of older patients from two randomized trials. J Clin Oncol 27:199–205
Kozloff MF, Sugrue M, Purdie DM, Flynn PJ, Kabbinavar F, Sargent D, Purdie DM, Dong W, Grothey A (2008) Safety and effectiveness of bevacizumab (BV) and chemotherapy (CT) in elderly patients (pts) with metastatic colorectal cancer (mCRC): results from the BRiTE observational cohort study. J Clin Oncol 26(15S):Abstract 4026
Saltz LB, Clarke S, Díaz-Rubio E, Scheithauer W, Figer A, Wong R, Koski S, Lichinitser M, Yang TS, Rivera F, Couture F, Sirzén F, Cassidy J (2008) Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: a randomized phase III study. J Clin Oncol 26:2013–2019
Scappaticci FA, Skillings JR, Holden SN, Gerber HP, Miller K, Kabbinavar F, Bergsland E, Ngai J, Holmgren E, Wang J, Hurwitz H (2007) Arterial thromboembolic events in patients with metastatic carcinoma treated with chemotherapy and bevacizumab. J Natl Cancer Inst 99:1232–1239
Silverstein MD, Heit JA, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ 3rd (1998) Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med 158:585–593
Acknowledgments
Medical writing/editing support was provided by Miller Medical Communications UK. The medical writing/editing support was funded by F. Hoffmann-La Roche.
Conflict of interest statement
This study was funded by Roche.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Cassidy, J., Saltz, L.B., Giantonio, B.J. et al. Effect of bevacizumab in older patients with metastatic colorectal cancer: pooled analysis of four randomized studies. J Cancer Res Clin Oncol 136, 737–743 (2010). https://doi.org/10.1007/s00432-009-0712-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-009-0712-3