
Abstract
The aim of the present paper was to examine the associations between anthropometric parameters, overweight, obesity, and socioeconomic status (SES) of children and adolescents in Poland. Data were collected in the “Elaboration of reference blood pressure ranges for children and adolescents in Poland” OLAF-PL0080 (OLAF) study, a nationally representative survey on growth and blood pressure references for children and adolescents aged 7–18 years. Body height, weight, and waist circumference (WC) were measured, and body mass index (BMI) was calculated. Anthropometric parameters were standardized for age and gender and expressed as z-scores. Statistical analyses were conducted on 10,950 children and adolescents whose parents provided socioeconomic questionnaires. The associations between anthropometric parameters, overweight (including obesity), and SES were analyzed using multiple regression and multiple logistic regression. The height was positively associated with higher levels of maternal education and, in the case of girls, also with paternal education. Higher level of income per capita, but not the highest, was associated with higher weight, BMI, and WC and, in the case of boys, also tall stature. The height, weight, BMI, and waist were significantly inversely associated with number of children in the family. Lower number of children in the family and higher level of income, but not the highest, increased odds of overweight and obesity. In the case of girls, the odds of obesity decreased with paternal higher level of education. Conclusion: The social position associated with parents’ education, better environment, and SES correlate with body height and weight of a child. However, it is associated with higher risk of overweight and abdominal obesity.
Similar content being viewed by others


Introduction
Body height and weight attained by children and adolescents during growth and development are sensitive indicators of an individual’s health and nutritional status, as well as a mirror of the country’s social and economic prosperity [24].
The biological development of humans has been the subject of research since the eighteenth century [22]. In 1833, the Belgian mathematician and anthropologist, Adolphe Quetelet, conducted a study in Brussels and was the first to conclude that socioeconomic factors can influence the size of newborns [21]. In the subsequent years of the nineteenth century, many studies were conducted on the development of children, including studies performed in Germany, France, and the USA [27]. In Poland, the physical development of children and adolescents has been the subject of study since the nineteenth century. Jędrzej Śniadecki, a pioneer in the field of physical education and child development, in his study entitled “On the physical education of a child” published in 1803, stressed the influence of a child’s environment on his or her development [23].
Research is being continued on the influence of the environment on the development of an individual and on achieving genetically determined potential. Studies point to place of residence, socioeconomic status (SES), and lifestyle as important factors affecting biological development and differentiating health in various stages of life [8, 9, 13, 17, 20, 26]. In Poland, significant changes in children’s height were observed in connection with social and economic transition during the second half of the twentieth century [3, 6]. Overweight and obesity prevalence among children increased in many countries. In Poland, overweight (including obesity) prevalence reached 20 % among primary school children [18]. Family SES is an important predictor of children’s overweight [2, 5, 16, 29].
The aim of the present paper was to examine the associations between anthropometric parameters, overweight, obesity, and SES of Polish children and adolescents aged 7–18 years.
Materials and methods
Study population and sampling
This study used data from the “Elaboration of reference blood pressure ranges for children and adolescents in Poland” OLAF-PL0080 (OLAF) study conducted by the Children’s Memorial Health Institute (CMHI) in cooperation with researchers nationwide. The study protocol was approved by the Bioethics Commission of the CMHI.
The studied population comprised school pupils aged 7 to 18 years, who between school years 2007–2008 and 2009–2010 attended primary, middle, and secondary schools located in all of Poland’s administrative regions. Participants were selected in a two-stage random sampling procedure. The primary sampling unit was a school sampled from an all-schools-in-Poland sampling frame provided by the Polish Ministry of Education. The schools were selected by stratified sampling with probability proportional to the size of the unit. In respect to primary and middle schools, the strata were urban/rural, whereas for secondary schools, the kind of school. In the second stage, the participants were randomly selected based on the number of pupils in a given school.
Data collection
Informed consent for participation in the study was obtained in writing from the parents of pupils under the age of 18 years, as well as from participants over the age of 16 years. Body height, body weight, and waist circumference (WC) were measured according to the procedures delineated in the OLAF study protocol and described previously [19]. Height was measured in duplicate using a stadiometer (SECA 214) in the standing position (with no shoes), to the nearest millimeter; if the difference between measurements exceeded 4 mm, a third measurement was taken. Body weight was measured in light underwear twice, using a digital, medical scale (Radwag WPT 100/200) and was recorded to the nearest 0.05 kg. In the case of a difference between measurements equal to or exceeding 0.3 kg, a third measurement was taken. Waist circumference was measured with anthropometric tape, in duplicate, to the nearest millimeter; in the case of a difference between measurements exceeding 3 cm, a third measurement was taken. Arithmetic averages of two or three height, weight, and WC measurements were analyzed. Body mass index was calculated as body weight divided by height in meters squared.
Age was calculated as the difference between the date of measurement and date of birth. The results were recorded as a decimal, and the midpoint of the age range was taken as the child’s age (e.g., children in the range ≥11.5 and <12.5 years were considered to be 12 years old).
Overweight and obesity were defined depending on gender and age using the BMI cutoffs according to the IOTF [10]. Data on SES and environment of a pupil were collected from questionnaires filled out by parents or an adult study participant. The questionnaire contained questions about maternal education, paternal education, household per capita monthly income, and number of children in the family. Dwelling, urban or rural, was determined on the basis of the school’s localization (urban/rural) in accordance with the Central Statistical Office (CSO) territorial classification. Only primary and middle schools were included in the dwelling analysis because almost all tertiary schools were located in urban areas.
Data inclusion and exclusion criteria
The data inclusion criteria were signed informed consent and age from 7 to 18 years. Exclusion from the analysis was lack of anthropometry measurements or SES data. Furthermore, data on weight and waist were excluded from pregnant women. There was no data exclusion based on health status of study participants.
Statistical analysis
Statistical analyses were performed separately for boys and girls using SAS 9.2 software. Height, weight, BMI, WC z-scores were calculated relative to the Polish 2010 growth references [18]. Data were grouped according to sex and socioeconomic categories and analyzed using descriptive statistics. SES variables were categorized into education: primary, vocational, secondary, and university; household monthly income per capita: ≤500 PLN, 501–1,000 PLN, 1,001–1,500 PLN, and >1,500 PLN; number of children in the family: one, two, three, four, or more; and dwelling: rural, urban. Final dummy variables were created for each, nonbinary SES variable category. The associations between continuous dependent variables: height, weight, BMI, waist (all variables expressed as z-scores), and independent SES variables were analyzed using forward stepwise multiple regression. In the multiple regression models, dwelling (rural/urban) was introduced, but due to the lack of statistical significance, it was not included in final regression models. A multivariable logistic regression analysis was performed with overweight (including obesity) and obesity as the dependent variables. In this analysis, dwelling also did not show statistically significant associations and was removed from the model. Values of p < 0.05 were considered significant.
Results
Among the 17,573 participants, 123 did not fulfill the age criteria (≥6.5 and <18.5 years). Seven women in the sample were pregnant, and their data on weight and waist, and consequently BMI, were excluded from the weight, BMI, and waist analysis, but kept for the height analysis. For the multivariate analysis, the number of participants was smaller due to missing data for SES characteristics: 459 for mother education, and/or 1,447 for father education, and/or 5,348 for income per capita, and/or 385 for number of children in the family. Thus, the sample, for the multivariable models, comprised 5,278 boys (48.2 %) and 5,672 girls. Height measurement was missing in the case of two boys, weight measurement was missing in the case of four boys and three girls, and waist measurement was missing in the case of three boys and six girls. Thus, final multivariable models concerning height, weight, BMI, and waist included 10,948, 10,943, 10,942, and 10,941 children and adolescents with complete data, respectively. The multivariable model with dwelling as independent variable included data from 8,247 primary and middle school pupils aged 7–15 years. Table 1 provides a summary of study sample dependent variable characteristics and sample size by sex and SES. Table 2 provides descriptive statistics of height, weight, BMI, waist z-score, and overweight and obesity prevalence according to the SES variables.
Parental education
Maternal secondary and university education were significantly positively associated with taller stature in both genders, whereas paternal secondary and university education were significantly positively associated with the height of girls (Table 3). In the case of boys, there was positive association between maternal secondary education and weight z-score. In the case of girls, the associations between maternal secondary education and WC, paternal secondary education and BMI, and paternal secondary and university education and WC were significantly inverse.
Income
Monthly income per capita higher than the lowest level reported by almost 50 % of study participants was significantly positively associated with weight, BMI, and waist in both genders. In the case of girls, height was not associated with income, whereas in the case of boys, there was a positive association between height and income in the range 501–1,000 PLN. The highest level of income was insignificantly associated with anthropometric variables (Table 3).
Number of children in the family
The height, weight, BMI, and waist were significantly inversely associated with number of children in the family (Table 3).
Dwelling (localization of school)
No significant associations were found for anthropometric variables, overweight and obesity prevalence, and dwelling in multivariable regression models.
Overweight and obesity
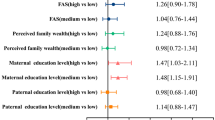
Maternal education was not associated with overweight and obesity in both genders. Higher levels of paternal education (secondary or university) significantly decreased odds of obesity in girls. Monthly income per capita higher than the lowest level increased odds of overweight and obesity in both genders. Although not significant, the highest income level was associated with lower risk of obesity among boys and girls and lower risk of overweight among girls. There was a strong, significant inverse relationship between risk of overweight (including obesity) and number of children in the family (Table 4).
Discussion
Our data confirm associations between basic anthropometric parameters of school-aged children and adolescents, overweight (including obesity), and many of the supposed SES determinants.
The qualitative differences among the analyzed indicators of physical development should be noted. Height is determined by the size of the skeletal system and does not change once the growth period is over. The values of three of the remaining parameters, weight, BMI, and WC, may undergo even short-term changes depending on nutrition, physical activity, and disease. BMI is a good indicator of the degree of an individual’s under- or overweight. Excessive weight has numerous negative health implications (arterial hypertension, type II diabetes, diseases of the musculoskeletal system, atherosclerosis and heart disease, psychological problems) [1, 7]. However BMI gives no indication of body fat distribution. It is WC that is an index of central adiposity both in adults and in children [25]. Central adiposity is related with a less favorable metabolic profile and is an important determinant of cardiovascular risk factor [11, 12].
We found differences in BMI, WC, and the prevalence of overweight and obesity depending on household per capita income, parental education, and family size. Analysis by gender showed that some socioeconomic factors may influence boys and girls differently, particularly in relation to WC and BMI. In Poland, according to the CSO, the average monthly household per capita income in 2008 was 1,046 PLN, i.e., about 250 Euro. In boys, above-average household per capita income was associated with significantly higher weight, WC, and BMI values, as well as higher risk of overweight including obesity; such a relationship was not found in girls. In the analysis of four levels of household per capita income, the lowest prevalence of overweight and obesity was found in boys from families with the lowest per capita monthly incomes, whereas in the case of girls—in families with the highest per capita monthly incomes.
It is noteworthy that children (both boys and girls) having more siblings had significantly lower BMI and WC values and a lower prevalence of overweight and obesity. This finding is in line with results from other studies [15].
Similar relationships of family size and level of parents’ education with greater height, weight, and BMI of young adults (19–20 years) were reported by researchers in Hungary, who also demonstrated a rise in average BMI over the studied period. Higher BMI values have been related, among others, to such variables as place of birth in the national capital and residence in a large city [14].
Education level, income, and place of residence are considered by some social-science theoreticians to be the basic factors forming a social structure. Factors modifying the physical development of children and adolescents may, therefore, be considered in relation to social stratification [4, 28]. The conducted analysis confirms that a higher social position of a family related to the higher parental education and higher SES contribute to the fuller development of genetic potential in terms of the height and weight of a child. It must, however, be stressed that a better economic situation may result in health hazards related to overweight and obesity. It is noteworthy that the prevalence of overweight and obesity increased with the monthly household per capita income, but not in the highest income group, in which it is especially noticeable in the case of girls; girls from the highest SES group were not only the tallest but also the thinnest.
Components of social status, such as parental education, income, place of residence, and family size, indirectly affect the development of the individual, with the commonly accepted direct stimuli being: the quality and quantity of food, morbidity, physical activity, health habits, and stress level.
Therefore, an important social and cultural factor influencing the physical development of children and adolescents is lifestyle, which is formed during socialization, as well as during later interactions of the individual, and is highly related to membership in a social class. This includes ways of interpreting social situations and patterns of everyday behavior. Lifestyle also comprises ways of eating and spending leisure time (including physical activity). A prohealth lifestyle that promotes the physical activity of the young generation requires an appropriate level of knowledge, motivation, and skills, as well as financial resources.
The anthropometric indicators of physical development considered above—height, weight, WC, and BMI—were analyzed in respect to one not isolated socioeconomic factor, whereas social variables are usually interrelated. In the studied group, there was a relationship between the level of parental education, monthly household per capita income, and family size.
Abbreviations
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- CMHI:
-
Children’s Memorial Health Institute
- IOTF:
-
International Obesity Task Force
- OLAF:
-
The “Elaboration of reference blood pressure ranges for children and adolescents in Poland” PL0080 study
- OR:
-
Odds ratio
- WC:
-
Waist circumference
References
Allock DM, Gardner MJ, Sowers JR (2009) Relation between childhood obesity and adult cardiovascular risk. Int J Pediatr Endocrinol 2009:108187
Andegiorgish AK, Wang J, Zhang X, Liu X, Zhu H (2012) Prevalence of overweight, obesity, and associated risk factors among school children and adolescents in Tianjin, China. Eur J Pediatr 171:697–703
Bielecki EM, Haas JD, Hulanicka B (2012) Secular changes in the height of Polish schoolboys from 1955 to 1988. Econ Hum Biol 10:310–317
Bielicki T, Malina MR, Waliszko H (1992) Monitoring the dynamics of social stratification: statural variation among polish conscripts in 1976 and 1986. Am J Hum Biol 4:345–352
Bielicki T, Szklarska A, Kozieł S, Welon Z (2000) Variation in the body mass index among young adult Polish males between 1965 and 1995. Int J Obes Relat Metab Disord 25:658–662
Bielicki T, Szklarska A, Kozieł S, Welon Z (2003) Political transformation in Poland in the light of anthropological research of 19-year-old males. Monografie Zakładu Antropologii Polskiej Akademii Nauk, Wrocław
Biro FM, Wien M (2010) Childhood obesity and adult morbidities. Am J Clin Nutr 91(Suppl):1499S–1505S
Bruner MW, Lawson J, Pickett W, Boyce W, Janssen I (2008) Rural Canadian adolescents are more likely to be obese compared with urban adolescents. Int J Pediatr Obes 3:205–211
Chen E, Martin AD, Matthews KA (2007) Trajectories of socioeconomic status across children’s lifetime predict health. Pediatrics 120:e297–e303
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH (2000) Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 320:1240–1243
Daniels SR, Morrison JA, Sprecher DL, Khoury P, Kimball TR (1999) Association of body mass distribution and cardiovascular risk factors in children and adolescents. Circulation 99:541–545
Flodmark CE, Sveger Y, Nilsson-Ehle P (1994) Waist measurement correlates to a potentially atherogenic lipoprotein profile in obese 12–14 year old children. Acta Paediatr 83:941–945
Goodman E (1999) The role of socioeconomic status gradients in explaining differences in US adolescents health. Am J Public Health 89:1522–1528
Gyenis G, Joubert K (2004) Socioeconomic determinants of anthropometric trends among Hungarian youth. Econ Hum Biol 2:321–333
Hunsberger M, Formisano A, Reisch LA, Bammann K, Moreno L, De Henauw S, Molnar D, Tornaritis M, Veidebaum T, Siani A, Lissner L (2012) Overweight in singletons compared to children with siblings: the IDEFICS study. Nutr Diabetes 2(7):e35
Kleiser C, Schaffrath Rosario A, Mensink GB, Prinz-Langenohl R, Kurth BM (2009) Potential determinants of obesity among children and adolescents in Germany: results from the cross-sectional KiGGS Study. BMC Public Health 2:9–46
Kobzová J, Vignerová J, Bláha P, Krejčovsky L, Riedlová J (2004) The 6th nationwide anthropological survey of children and adolescents in the Czech Republic in 2001. Cent Eur J Public Health 12:126–130
Kułaga Z, Litwin M, Tkaczyk M, Palczewska I, Zajączkowska M, Zwolińska D, Krynicki T, Wasilewska A, Moczulska A, Morawiec-Knysak A, Barwicka K, Grajda A, Gurzkowska B, Napieralska E, Pan H (2011) Polish 2010 growth references for school-aged children and adolescents. Eur J Pediatr 170:599–609
Kułaga Z, Litwin M, Tkaczyk M, Różdżyńska A, Barwicka K, Grajda A, Świąder A, Gurzkowska B, Napieralska E, Pan H (2010) The height-, weight-, and BMI-for-age of Polish school-aged children and adolescents relative to international and local growth references. BioMed Central Public Health 10:109
Liu J, Bennett KJ, Harun N, Probst JC (2008) Urban–rural differences in overweight status and physical inactivity among US children aged 10–17 years. J Rural Health 24:407–415
Quetelet A (1835) Sur I’homme et le development des faculties, ou essai de physique sociale. Paris 2:34–62
Roederer JG (1753) Serme de Pandere et Longitudinae Infantum Recens Natorum. Akad Wiss Gottingensis 3:410–424
Śniadecki J (1805/1806) On the physical education of a child. Dziennik Wileński T. 2 nr 41
Tanner JM (1986) Growth as a mirror of the condition of society: secular trend and class distinction. In: Demirjian A, Brault-Dubuc M (eds) Human growth: a multidisciplinary review. Taylor and Francis, London, pp 3–34
Taylor RW, Jones IE, Williams SM, Goulding A (2000) Evaluation of waist circumference, waist-to hip ratio, and conicity index as screening for high trunk fat mass, as measured by dual-energy X-ray absorptiometry in children aged 3–19 y. Am J Clin Nutr 72:490–495
Wang Y (2010) Cross-national comparison of childhood obesity: the epidemic and the relationship between obesity and socioeconomic status. Int J Epidemiol 30:1129–1136
Ward WP (1998) The biological standard of living in comparative perspective. In: Komlos J, Baten J (eds) Birth weight and the history of modern biological living standards. Franz Steiner, Stuttgart, pp 303–305
Weber G, Seidler H, Wilfing H, Hauser G (1995) Secular change in Austria: an effect of population stratification? Ann Hum Biol 22:277–288
Ządzińska E, Rosset I, Kozieł S, Nawarycz T, Borowska-Strugińska B, Lorkiewicz W, Ostrowska-Nawarycz L, Sitek A (2012) Frequency of under- and overweight among children and adolescents during the economic transition in Poland. Homo 63:216–232
Acknowledgments
The OLAF study was supported by a grant from Iceland, Liechtenstein, and Norway through the EEA Financial Mechanism and the Norwegian Financial Mechanism, and the Ministry of Science and Higher Education of Poland (grant number PL0080).
The OLAF Study Group: Medical University of Białystok: Agnieszka Rybi-Szumińska, Michał Szumiński, Katarzyna Taranta-Janusz, Edyta Tenderenda, Anna Wasilewska; Regional Children’s Hospital in Bydgoszcz: Beata Jasińska; Medical University of Gdańsk: Piotr Czarniak, Dominik Świętoń, Przemysław Szcześniak; Jagiellonian University Medical College in Kraków: Monika Miklaszewska, Anna Moczulska, Katarzyna Wilkosz, Katarzyna Zachwieja, Iwona Ogarek; Medical University of Lublin: Marek Majewski, Aleksandra Sobieszczańska-Droździel, Izabela Szlązak, Paweł Szlązak, Małgorzata Zajączkowska; Polish Mother’s Memorial Hospital Research Institute in Łódź: Monika Pawlak-Bratkowska, Anna Półtorak-Krawczyk, Marcin Tkaczyk; District Hospital in Kędzierzyn-Koźle: Danuta Gmyrek; Poznan University of Medical Sciences: Tomasz Krynicki, Jolanta Sołtysiak; Regional Children’s Hospital in Toruń: Roman Stankiewicz, Sława Zbucka; The Children’s Memorial Health Institute in Warszawa: Robert Pietruczuk, Agnieszka Różdżyńska-Świątkowska, Jan Szpor; Wroclaw Medical University: Jacek Kleszczyński, Magdalena Naleśniak, Anna Wawro, Irena Wikiera-Magott, Danuta Zwolińska; Medical University of Silesia: Piotr Adamczyk, Tatiana Augustyn-Iwachów, Beata Banaszak, Omar Bjanid, Katarzyna Broll-Waśka, Aurelia Morawiec-Knysak.
We would like to thank Dr Piotr Wójcik from the Faculty of Economic Sciences of the University of Warsaw for the consultation of the multiple regression models used in the data analysis.
Conflict of interest
The authors declare that they have no personal financial relationships with the organizations sponsoring the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article
Cite this article
Gurzkowska, B., Kułaga, Z., Litwin, M. et al. The relationship between selected socioeconomic factors and basic anthropometric parameters of school-aged children and adolescents in Poland. Eur J Pediatr 173, 45–52 (2014). https://doi.org/10.1007/s00431-013-2109-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-013-2109-1