
Abstract
Preventing ventilator-associated pneumonia (VAP) is one of the Department of Health Saving Lives initiatives. We describe the institution of a purpose-designed bundle of care in a tertiary paediatric ICU based on the available literature as part of our hospital’s transformation project into reducing health-care-associated infection. A nurse-led VAP surveillance programme is in place, and we used this to compare VAP incidence before and after commencing a series of care measures aimed at reducing VAP as part of an overall drive for patient safety. The diagnostic criteria, surveillance methods and rates of VAP (5.6 per 1,000 ventilator days) have been previously reported. Nurse educators were added to the original core group, as a key feature is buy in from nursing staff. All nursing staff had multiple training opportunities, and VAP project education became a routine part of staff induction. The major features of the bundle of care were (1) elevation of bed to maximum (target, 45°; however, no beds currently permit this so achieved 20–30°), (2) mouth care using chlorhexidine or tooth brushing, (3) clean suctioning practice, (4) all patients not on full feeds commenced on ranitidine and (5) 4-hourly documentation. Compliance with these aspects was monitored. After the institution of the bundle, no paediatric case of VAP was recorded over a 12-month period, according to a priori definitions. One adult patient had a confirmed VAP over the same time interval. A paediatric VAP bundle was associated with reduced VAP on a UK PICU.
Similar content being viewed by others


Introduction
The safety of children within our hospitals is increasingly an area of focus for all involved in child health. Ventilator-associated pneumonia (VAP) is the second most common health-care-associated infection (HCAI) in paediatric intensive care (PICU) accounting for 20% of nosocomial infections [14, 19]. VAP is defined as a pneumonia developing later than 48 h after intubation and initiation of mechanical ventilation [28] and has been linked to increased morbidity, mortality [2, 15, 18] and costs [15, 19].
VAP risk increases with duration of mechanical ventilation, rates being expressed as infectious episodes per 1,000 ventilator days. Prevalence ranges from 2.9 to 11.6/1,000 ventilator days [2, 15] although data in children remain limited.
Early-onset paediatric VAP classically occurs within 5 days of intubation, is associated with aspiration of gastric contents and is usually due to fully sensitive organisms [26, 33]. Late-onset VAP occurs after 5 days of intubation and characteristically is caused by multi-resistant organisms [32].
Paediatric studies have implicated immunodeficiency, syndromes associated with neuromuscular weakness, transport off PICU, re-intubation, female gender, post surgical diagnosis, narcotic use and the use of enteral feeds as independent risk factors [2, 15, 36].
Historically, HCAIs have been viewed as an inevitable consequence of critical illness, but increasingly are acknowledged as avoidable adverse health-care events and are certain to feature in the new UK Commissioning for Quality and Innovation payment frameworks for PICU. The business case for preventing VAP has been made and is clear [5].
However, whilst VAP prevention is a core element of campaigns such as the US 5 Million Lives campaign and the Department of Health Saving Lives initiative [9], concerns have been raised about the suitability of such generic programmes to PICU [8]. For this reason, we established an a priori UK VAP surveillance programme and bundle of care in an attempt to reduce PICU VAP.
In 2006–2007 when this programme was established, the CDC definition for VAP excluded pneumonia occurring <48 h after intubation [20]; this 48-h rule was removed in 2007 [6]. The establishment of VAP surveillance in our unit has been previously reported [35] and occurred over a 3-month period showing a VAP rate of 5.6 per 1,000 ventilator days. The surveillance was stopped as it was felt to extend when others had reported successful reduction with bundles of care was unethical.
A paediatric specific VAP group (ICU physician, senior ICU nurse, physiotherapist and microbiologist) was established and an agreed definition of paediatric VAP devised after literature review. This was because existing CDC definitions did not seem applicable to the patient population in the unit in question, with a large proportion of immunocompromised children, few bronchoscopies in the patient group and no specific leukocyte definitions in the CDC definition.
Although successful bundle-related reduction of VAP has been described in the USA [4], this paper describes the first reduction of paediatric VAP in the UK following implementation of a novel bundle of care.
Methods
As this study was deemed quality improvement rather than human subjects research, institutional review board was not required.
Inclusion
All invasively ventilated patients admitted to paediatric intensive care between January 2008 and December 2009 (12 months) were included in the study.
Exclusion
Patients who were ventilated <48 h, non-invasively ventilated or who died within 48 h of ventilation were excluded from the study. For this study, the VAP group (ICU physician, senior ICU nurse, physiotherapist and microbiologist) were joined by PICU practice educators and members of the Trust’s transformation team.
Surveillance
Active VAP surveillance continued throughout the study with a flow diagram (Fig. 1) at each bed space to facilitate investigations, including daily full blood counts and, if indicated, sputum samples and blood cultures with temperatures ≥38.5°C or <36.0°C. The bedside nurse was responsible for collecting VAP data over the 12-month period until 24 h post extubation, discharge or death.

PICU surveillance process for VAP
Radiological
Admission chest X-rays (CXRs) are standard for ventilated transfers into PICU, and post intubation CXR routine; therefore, all children had an initial baseline intubated CXR.
Routine daily X-rays are not performed, so only X-rays requested by clinicians were examined. A senior physiotherapist, who had undergone specific training, reviewed all CXRs taken over the 1-year period, and any new changes led to VAP screening by secretion sampling and notification to microbiology. All X-rays were reported by attending radiologists and reviewed daily by the physiotherapist and ICU team providing another point for possible VAP triggering.
Clinical
-
1.
New onset or worsening of bronchopurulent secretions:
Purulence of bronchial secretions is traditionally a quantitative laboratory diagnosis, though many laboratories report it qualitatively (i.e. purulent+++, epithelials−), and bedside clinical descriptions can be variable. Nurses and clinicians sent sputum to the laboratory if there was a change in colour or offensive smell to the sputum, clinical concern about chest infection or if triggered by screening.
Furthermore, clinical infection ‘workup’ samples were reviewed including bronchoalveolar lavage, pleural fluid and lung biopsy, though only sputum samples were sent after ‘possible VAP’ trigger.
-
2.
Bloods
Daily full blood count and C-reactive protein (CRP) are sent in PICU during periods of invasive multiple-organ support. In stable patients, bloods are triggered for clinical reasons, such as infection screening due to temperature, new CXR changes or secretions suggestive of infection. No bloods were sent purely for the VAP project. Elevated CRP triggered screening of secretions, but was not part of VAP diagnostic criteria.
-
3.
Temperature
Bedside nurses’ screening of all patients for hyper/hypothermia was validated by the nurse in charge at the end of each 12-h shift and entered into the purpose-designed section of the electronic bedside record.
GOSH diagnostic criteria for VAP
VAP was defined for all ages as pneumonia occurring >48 h after intubation diagnosed by specific chest radiograph (CXR) changes with at least three clinical or laboratory findings (Table 1).
Radiological
VAP was suggested by new or progressive pulmonary infiltrates, consolidation or cavitation (Fig. 1) on at least two serial CXRs with gradual resolution (rapid resolution suggests non-infective aetiology, e.g. pulmonary oedema or atelectasis).
Clinical
Core temperature ≥38.5°C or <36°C
Hyper/Hypothermia was defined as at least two consecutive abnormal readings, using standard measurement techniques, in a 24-h period not clearly attributable to extra-pulmonary infection, the environment or blood/drug reactions.
Laboratory
Leucopenia or leucocytosis
was defined by age according to the International Consensus Conference on Pediatric Sepsis statement [23].
Significant culture of respiratory secretions
Microbial growth from endotracheal secretions, or when performed bronchiolar lavage, was reported semi-quantitatively using calibrated loops according to standard operating procedures in the microbiology department. Sensitivities were performed on any potential respiratory pathogen.
Relevant culture from alternative site of infection
Positive blood cultures of likely respiratory tract pathogens, unrelated to another source of infection, were considered in the diagnosis of VAP, as were significant cultures from pleural fluid and lung parenchyma biopsy, or pathogens detected by validated immunofluorescence.
Immunocompromised children required the same CXR changes, but only two clinical or laboratory findings because leucopenia/leucocytosis is unreliable in this group. Children were categorised as immunocompromised with any of neutropenia (count <1.0 × 109∧/L], HIV, chemotherapy, leukaemia/lymphoma/post bone marrow transplant, post splenectomy, immunosuppressive drugs (long-term steroids (any dose >7 days), azathioprine, ciclosporin, mycophenolate mofetil, tacrolimus, methotrexate, anti-TNF).
Bundle of care
The available literature was reviewed, and an appropriate bundle of care designed, (Fig. 2) with an emphasis on simple and cost-neutral interventions with minimal potential complications. For this reason, selective decontamination was not part of the initial bundle.

VAP care bundle placed at every PICU bedspace
Sedation policy change was not considered at this stage, as a separate interventional study is planned. Although remifentanil became standard for head injuries between initial surveillance and bundle introduction, none of the original VAP series were trauma patients. Several education sessions for ICU nurses were held and now form part of routine induction.
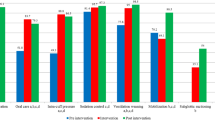
Compliance with the bundle was stringently monitored throughout and reported monthly. Care bundle aspects were audited individually to identify compliance lapses and enable targeted steps to improve overall compliance, which was only awarded if all aspects were consistently delivered for 24 h (Fig. 3). Regular interactive VAP meetings and continuing dialogue with bedside and senior nurses highlighted compliance barriers and allowed adjustments to the care bundles, which played a fundamental role in the project’s success. One example was a mouth care protocol alteration following feedback from nursing staff concerned about bundle-generated sleep deprivation (Fig. 4).

Progression of compliance and alteration to bundle

Mouth care component of bundle of care
Results
Bundle compliance increased progressively throughout the study (Fig. 3). There were 730 admissions during the study period of which 448 were ventilated for >24 h. Fifteen cases were triggered for review.
No paediatric cases of VAP were detected during the year. One adult patient, (>16 years) admitted to PICU with severe adult respiratory distress syndrome following post-operative aspiration during recovery from elective high-risk surgery, had Escherichia coli VAP diagnosed on day 7. The patient survived to discharge, but died from neurological complications within 28 days.
If the earlier or later US Centers for Disease Control definitions are used, the same overall result for the year of post bundle implementation is achieved, although the later CDC definition would lead to a higher pre-bundle rate due to the presence of two children with VAP in the first 48 h of admission. Paediatric VAP rate was 0 per 1,000 ventilator days, and total VAP rate was 0.04/1,000 ventilator days.
To encourage staff participation and a sense of ownership, monthly VAP incidence and bundle compliance were fed back to staff via a dedicated VAP notice board on PICU.
Discussion
There are few publications in regard to HCAI in UK paediatric and neonatal intensive care, especially using improvement methodologies. Indeed, few units publish infection rates per se despite this being information on which standards might be judged by commissioners and families. Matching Michigan [34], the UK National Patient Safety Agency project aimed at providing a uniform ‘minimal’ achievable rate for central line infections, offers a chance to reduce that HCAI rate nationally. VAP should surely soon be subject to a similar process, and we present a successful UK project in which VAP incidence in PICU has been reduced.
It is accepted that quality improvement activities ‘are not human subjects research and should not undergo review by an institutional review board’, so such activities are part of professional supervision of clinical practice [29].
This study uses a novel paediatric definition for VAP, designed in the absence of a satisfactorily accepted definition in 2007. Surveillance using this definition revealed VAP on the unit in question, a busy tertiary non-cardiac PICU with a relatively high proportion of immunosuppressed children. The introduction of a bundle of care, comparable to similar bundles, is described, and reduction in VAP rates reported—though rather early to be fully ascribed only to bundle implementation.
The surveillance practised during the study has already been described [35] and has been driven by an attempt to remain minimally invasive and workable in a busy acute unit.
Obtaining minimally contaminated respiratory cultures from children is challenging. Bronchoscopic techniques, used in adult surveillance, are not routine in UK PICU, and whilst blind bronchoalveolar lavage and protected brush samples are reliable, reproducible, diagnostic tools, the former is associated with pneumothorax and raised intracranial pressure whilst the latter has high false-negative rates with relatively high antibiotic use [21]. Tracheal aspirates are sensitive for VAP, and any lack of specificity due to upper respiratory tract pathogen contamination is arguably outweighed by the advantage of rapid safe bedside sampling.
Radiographic evidence is only 50–75% sensitive for paediatric pneumonia [39] as differentiating atelectasis and consolidation is difficult, so pulmonary contusions, interstitial lung disease or community-acquired pneumonia can be mistaken for VAP without peri-admission CXR [32].
Immunocompromised children required the same CXR changes, but only two clinical or laboratory findings as leucopenia/leucocytosis in this group are unreliable [20]. Whilst the bundle of care was designed for the unit in question, all components are generic and could easily be applied elsewhere. The components were specifically selected for ease of implementation, simplicity of surveillance of use and minimum potential side effects to individual children and the unit overall.
Elevation of bed head is an accepted component of VAP elimination [25] with a suggestion of 45° being optimal. None of the beds in our unit has this mechanical level of elevation, and hence, the bundle suggested maximum achievable elevation, effectively around 20–30°.
The role of gastro-oesophageal reflux in paediatric VAP is controversial, with some authors suggesting a causal link from the use of antacid therapy [13], whereas others have demonstrated increased VAP incidence with both alkaline and acid reflux, the latter having a significant mortality association, but with a relatively high underlying prevalence meaning any extrapolation be guarded [1]. We chose to use anti-reflux treatment in our bundle, not because of this risk, but to avoid gastric erosions per se with the largest randomized adult study suggesting this to be effective and not associated with VAP [7]. Ranitidine, or omeprazole if otherwise indicated, was given to any patient not tolerating full enteral feeds.
An established relationship exists between VAP and aspiration of colonised oropharyngeal secretions [3]. Factors contributing to colonisation include pH-altering drugs that permit overgrowth of gastric bacteria and feeding tubes that encourage bacterial migration [32]. Micro-aspiration of colonised secretions occurs because of inadequate glottic closure around endotracheal tubes (ETT) and also because neuromuscular-blocking and sedative agents impair cough and mucociliary clearance, especially in those nursed supine [12, 24]. Suctioning has also been implicated in VAP through direct contamination due to inadequate hand washing, oro/nasopharyngeal suctioning followed by ETT suction and from mucosal trauma due to deep suctioning [27]. ETT colonisation is known to occur early after intubation [17], and theoretically, suctioning might dislodge bacteria into the lower airways. Significantly, colonisation occurs first in the oropharynx and stomach, followed by lower airways and finally the ETT suggesting aspiration, rather than contaminated equipment, may be implicated in VAP [3, 22].
The theory of retrograde contamination of the endotracheal tube from the oropharynx suggests the effectiveness of oral sterilization techniques. Oral hygiene is an important component in VAP prevention, with both mechanical and pharmacological interventions recommended [30] to reduce the bacteria load in the oral cavity. Mechanical interventions include tooth brushing and rinsing of the oral cavity with thorough suctioning of secretions, which removes the bacteria in dental plaque. Pharmacological interventions include the use of antimicrobial agents, with twice daily chlorhexidine oral rinse shown to decrease VAP by decreasing colonisation in adults undergoing cardiac surgery [10]. The mouth care component of our bundle consisted of 4-hourly chlorhexidine mouthwash, or 12-hourly tooth brushing in children with teeth.
Aspiration of secretions and the use of contaminated equipment are established risk factors for VAP. To minimise distress to the patient, endotracheal suction was performed when clinically indicated, but universal precautions were utilised together with stringent hand washing pre and post each suction procedure. Care was also taken to prevent the condensate from entering the airway, with the ventilator tubing being checked hourly.
Whilst immunosuppression has been shown in one paediatric prospective cohort study [16] to be an independent predictor of VAP, our initial surveillance showed no VAP in this group, and now no cases over 16 months of active surveillance. This may be due to the unit practice of preferring non-invasive ventilation in such children, including perceived high-risk bone marrow transplant admissions.
In our pre-bundle surveillance, some children [35] fulfilled VAP criteria, but within the first 48 h of intubation, and were excluded by our definitions. This intubation-associated pneumonia (IAP)—although some use the term to describe early VAP [38]—is conceivably due to peri-intubation aspiration of contaminated secretions. Though not included in this study surveillance, clinical staff did not report any cases over the 12 months. Clearly a bundle like ours, targeted at traditional theories of VAP pathogenesis [3], is unlikely to impact on IAP, which we consider a separate entity, and specific attention to this entity is urgently warranted.
Selective decontamination is, arguably, the most evidence-based single component of VAP reduction in adult practice [11]; however, concerns over potential antibiotic resistance [31] mean SDD introduction should be accompanied by unit background surveillance which has funding implications outside the remit of this project.
One interesting finding is the virtual elimination of detectable VAP from our unit before reasonably complete bundle compliance. Whether this suggests some components are more important than others, or as we consider, is perhaps due to the Hawthorne effect, arguably those no longer exposed to VAP and the health-care commissioners are surely more concerned with the overall infection reduction.
No increase in VAP incidence occurs if our annual data are analysed with either new or old CDC definitions instead of out purpose-designed paediatric VAP definition. Whether this represents a failure of current definitions or successful bundle effect requires further work. Our a priori VAP definition can be criticized in terms of novelty, though no accepted paediatric VAP definition existed at the onset of our VAP project, nor does. A consensus international definition of paediatric VAP is surely necessary.
Staff engagement
Ensuring a busy PICU adopts a specific improvement methodology can be a challenge. Both nursing and medical staff together with unit administrators and Trust managers must engage in such processes fully to ensure successful adoption.
We adopted the ‘Seven categories that influence change in practice’ [37] at the project outset, and the rational for change was explained to all groups early in sessions facilitated by practice educators. Regular consistent communication across the unit occurred via a dedicated VAP board on PICU, with latest VAP rates and bundle compliance updated regularly. Specific supportive feedback was given to individual nurses to enable consistency of implementation of continued screening and the bundle itself. Overall, this approach enabled significant ‘buy in’ from the most critical team members for this project, the nursing staff.
Conclusion
We have demonstrated successful reduction of ventilator-acquired pneumonia in a tertiary PICU using a purpose-designed bundle of care, to rates much lower than usually reported in the literature. Further work to assess IAP and selective decontamination of the gastro-intestinal tract with full unit background surveillance, together with changes in sedative practices, are planned. Our one case, whilst outside our a priori definitions, is one case too many.
References
Abdel-Gawad T, El Hodhod M, Ibrahim H, Michael Y (2009) Gastroesophageal reflux in mechanically ventilated pediatric patients and its relation to ventilator-associated pneumonia. Crit Care 13:R164
Almuneef M, Memish ZA, Balkhy HH, Alalem H, Abutaleb A (2004) Ventilator-associated pneumonia in a pediatric intensive care unit in Saudi Arabia: a 30-month prospective surveillance. Infect Control Hosp Epidemiol 25:753–758
Berdal JE, Bjornholt J, Blomfeldt A, Smith-Erichsen N, Bukholm G (2007) Patterns and dynamics of airway colonisation in mechanically-ventilated patients. Clin Microbiol Infect 13:476–480
Bigham MT, Amato R, Bondurrant P, Fridriksson J, Krawczeski CD, Raake J, Ryckman S, Schwartz S, Shaw J, Wells D, Brilli RJ (2009) Ventilator-associated pneumonia in the pediatric intensive care unit: characterizing the problem and implementing a sustainable solution. J Pediatr 154:582–587
Brilli RJ, Sparling KW, Lake MR, Butcher J, Myers SS, Clark MD, Helpling A, Stutler ME (2008) The business case for preventing ventilator-associated pneumonia in pediatric intensive care unit patients. Jt Comm J Qual Patient Saf 34:629–638
Centers for Disease Control and Prevention (2011) Protocols and definitions for the ventilator-associated pneumonia option of the device-associated module of the patient safety component of the NHSN . Page Office of the Associate Director for Communication, Division of News and Electronic Media. Ref Type: Internet Communication
Cook D, Guyatt G, Marshall J, Leasa D, Fuller H, Hall R, Peters S, Rutledge F, Griffith L, McLellan A, Wood G, Kirby A, Tweeddale M, Pagliarello J, Johnston R, The Canadian Critical Care Trials Group (1998) A Comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. N Engl J Med 338:791–797
Curley MA, Schwalenstocker E, Deshpande JK, Ganser CC, Bertoch D, Brandon J, Kurtin P (2006) Tailoring the Institute for Health Care Improvement 100,000 Lives Campaign to pediatric settings: the example of ventilator-associated pneumonia. Pediatr Clin North Am 53:1231–1251
Department of Health (2006) The Health Act 2006—code of practice for the prevention and control of healthcare associated infections. Department of Health, London, Ref Type: Generic
DeRiso AJ, Ladowski JS, Dillon TA, Justice JW, Peterson AC (1996) Chlorhexidine gluconate 0.12% oral rinse reduces the incidence of total nosocomial respiratory infection and nonprophylactic systemic antibiotic use in patients undergoing heart surgery. Chest 109:1556–1561
de Smet AM, Kluytmans JA, Cooper BS, Mascini EM, Benus RF, van der Werf TS, van der Hoeven JG, Pickkers P, Bogaers-Hofman D, van der Meer NJ, Bernards AT, Kuijper EJ, Joore JC, Leverstein-van Hall MA, Bindels AJ, Jansz AR, Wesselink RM, de Jongh BM, Dennesen PJ, van Asselt GJ, te Velde LF, Frenay IH, Kaasjager K, Bosch FH, van Iterson M, Thijsen SF, Kluge GH, Pauw W, de Vries JW, Kaan JA, Arends JP, Aarts LP, Sturm PD, Harinck HI, Voss A, Uijtendaal EV, Blok HE, Thieme Groen ES, Pouw ME, Kalkman CJ, Bonten MJ (2009) Decontamination of the digestive tract and oropharynx in ICU patients. N Engl J Med 360:20–31
Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M (1999) Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet 354:1851–1858
du Moulin GC, Paterson DG, Hedley-Whyte J, Lisbon A (1982) Aspiration of gastric bacteria in antacid-treated patients: a frequent cause of postoperative colonisation of the airway. Lancet 1:242–245
Elward AM (2003) Pediatric ventilator-associated pneumonia. Pediatr Infect Dis J 22:445–446
Elward AM, Warren DK, Fraser VJ (2002) Ventilator-associated pneumonia in pediatric intensive care unit patients: risk factors and outcomes. Pediatrics 109:758–764
Fayon MJ, Tucci M, Lacroix J, Farrell CA, Gauthier M, Lafleur L, Nadeau D (1997) Nosocomial pneumonia and tracheitis in a pediatric intensive care unit: a prospective study. Am J Respir Crit Care Med 155:162–169
Feldman C, Kassel M, Cantrell J, Kaka S, Morar R, Goolam MA, Philips JI (1999) The presence and sequence of endotracheal tube colonization in patients undergoing mechanical ventilation. Eur Respir J 13:546–551
Fischer JE, Allen P, Fanconi S (2000) Delay of extubation in neonates and children after cardiac surgery: impact of ventilator-associated pneumonia. Intensive Care Med 26:942–949
Foglia E, Meier MD, Elward A (2007) Ventilator-associated pneumonia in neonatal and pediatric intensive care unit patients. Clin Microbiol Rev 20:409–425, table
Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM (1988) CDC definitions for nosocomial infections, 1988. Am J Infect Control 16:128–140
Gauvin F, Dassa C, Chaibou M, Proulx F, Farrell CA, Lacroix J (2003) Ventilator-associated pneumonia in intubated children: comparison of different diagnostic methods. Pediatr Crit Care Med 4:437–443
George DL, Falk PS, Wunderink RG, Leeper KV Jr, Meduri GU, Steere EL, Corbett CE, Mayhall CG (1998) Epidemiology of ventilator-acquired pneumonia based on protected bronchoscopic sampling. Am J Respir Crit Care Med 158:1839–1847
Goldstein B, Giroir B, Randolph A (2005) International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med 6:2–8
Hampton DC, Griffith D, Howard A (2005) Evidence-based clinical improvement for mechanically ventilated patients. Rehabil Nurs 30:160–165
Hess DR (2005) Patient positioning and ventilator-associated pneumonia. Respir Care 50:892–898
Kollef MH, Shorr A, Tabak YP, Gupta V, Liu LZ, Johannes RS (2005) Epidemiology and outcomes of health-care-associated pneumonia: results from a large US database of culture-positive pneumonia. Chest 128:3854–3862
Kunis KaPK (2003) Ventilator-associated pneumonia in the ICU: its pathophysiology, risk factors and prevention. Am J of Nursing 103(8):64AA–64GG, Ref Type: Generic
Langley JM, Bradley JS (2005) Defining pneumonia in critically ill infants and children. Pediatr Crit Care Med 6:S9–S13
Lynn J, Baily MA, Bottrell M, Jennings B, Levine RJ, Davidoff F, Casarett D, Corrigan J, Fox E, Wynia MK, Agich GJ, O’Kane M, Speroff T, Schyve P, Batalden P, Tunis S, Berlinger N, Cronenwett L, Fitzmaurice JM, Dubler NN, James B (2007) The ethics of using quality improvement methods in health care. Ann Intern Med 146:666–673
Munro CL, Grap MJ, Elswick RK Jr, McKinney J, Sessler CN, Hummel RS III (2006) Oral health status and development of ventilator-associated pneumonia: a descriptive study. Am J Crit Care 15:453–460
Oostdijk EA, de Smet AM, Blok HE, Thieme Groen ES, van Asselt GJ, Benus RF, Bernards SA, Frenay IH, Jansz AR, de Jongh BM, Kaan JA, Leverstein-van Hall MA, Mascini EM, Pauw W, Sturm PD, Thijsen SF, Kluytmans JA, Bonten MJ (2010) Ecological effects of selective decontamination on resistant gram-negative bacterial colonization. Am J Respir Crit Care Med 181:452–457
Pieracci FM, Barie PS (2007) Strategies in the prevention and management of ventilator-associated pneumonia. Am Surg 73:419–432
Richards MJ, Edwards JR, Culver DH, Gaynes RP (1999) Nosocomial infections in pediatric intensive care units in the United States. National Nosocomial Infections Surveillance System. Pediatrics 103:e39
Richardson A (2009) Minimising central venous catheter-associated bloodstream infections–‘Matching Michigan’ in England. Nurs Crit Care 14:105–106
Richardson M, Hines S, Dixon G, Highe L, Brierley J (2010) Establishing nurse-led ventilator-associated pneumonia surveillance in paediatric intensive care. J Hosp Infect 75:220–224
Srinivasan R, Asselin J, Gildengorin G, Wiener-Kronish J, Flori HR (2009) A prospective study of ventilator-associated pneumonia in children. Pediatrics 123:1108–1115
Stevens B, Lee SK, Law MP, Yamada J (2007) A qualitative examination of changing practice in Canadian neonatal intensive care units. J Eval Clin Pract 13:287–294
Torres A, Ewig S, Lode H, Carlet J (2009) Defining, treating and preventing hospital acquired pneumonia: European perspective. Intensive Care Med 35:9–29
Wright ML, Romano MJ (2006) Ventilator-associated pneumonia in children. Semin Pediatr Infect Dis 17:58–64
Acknowledgements
We would like to thank the GOSH transformation team, especially Olivia Waller, together with Sisters Sharon Chalkley and Yvette Harding, and all the nursing staff of GOSH PICU whose enthusiasm and dedication have enabled the success of this project.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brierley, J., Highe, L., Hines, S. et al. Reducing VAP by instituting a care bundle using improvement methodology in a UK Paediatric Intensive Care Unit. Eur J Pediatr 171, 323–330 (2012). https://doi.org/10.1007/s00431-011-1538-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-011-1538-y