
Abstract
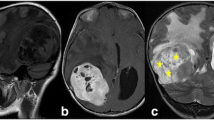
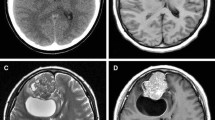
We describe an unusual progression of astrocytoma into secondary glioblastoma exhibiting advanced neuronal immunophenotype. A tumor of the left frontal lobe of a 35-year-old man was diagnosed as astrocytoma. The tumor was treated by partial removal with postoperative chemoradiotherapy, followed by extensive removal of the residual regrowing tumor 5 month later. A secondary tumor was discovered and partially resected 8 years later, but the patient died 11 months following the operation due to extensive tumor progression showing subarachnoidal and intraventricular dissemination. The secondary tumor was small cell-predominant, highly proliferative tumor with an extremely high MIB-1 labeling index (80%). Unexpectedly, most of the tumor cells were positive for neuronal markers (synaptophysin and NeuN), but not for glial fibrillary acidic protein (GFAP). Retrospective examination of the original tumor revealed not only diffuse GFAP expression, but also neuronal marker expressions in small numbers of tumor cells that were hard to discriminate from the other cells on hematoxylin-eosin (HE) stain. This way of malignant progression of astrocytoma was quite unusual. Although the secondary tumor was classified as glioblastoma according to World Health Organization (WHO) classification (2000), it might be categorized into new variants of malignant glioneuronal tumors proposed recently.


Similar content being viewed by others

References
Alvarez-Buylla A, Garcia-Verdugo JM, Tramontin AD (2001) A unified hypothesis on the lineage of neural stem cells. Nat Rev Neurosci 2:287–293
Arita N, Taneda M, Hayakawa T (1994) Leptomeningeal dissemination of malignant gliomas. Incidence, diagnosis and outcome. Acta Neurochir (Wien) 126:84–92
Burger PC, Pearl DK, Aldape K, Yates AJ, Scheithauer BW, Passe SM, Jenkins RB, James CD (2001) Small cell architecture-a histological equivalent of EGFR amplification in glioblastoma multiforme? J Neuropathol Exp Neurol 60:1099–1104
Cenacchi G, Giangaspero F (2004) Emerning tumor entities and variants of CNS neoplasms. J Neuropathol Exp Neurol 63:185–192
Franke FE, Schachenmayr W, Osborn M, Altmannsberger M (1991) Unexpected immunoreactivities of intermediate filament antibodies in human brain and brain tumors. Am J Pathol 139:67–79
Hassoun J, Soylemezoglu F, Gambarelli D, Figarella-Branger D, von Ammon K, Kleihues P (1993) Central neurocytoma: a synopsis of clinical and histological features. Brain Pathol 3:297–306
Hirato J, Nakazato Y, Ogawa A (1994) Expression of non-glial intermediate filament proteins in gliomas. Clin Neuropathol 13:1–11
Kleihues P, Burger PC, Collins VP, Newcomb EW, Ohgaki H, Cavenee WK (2000) Glioblastoma. In: Kleihues P, Cavenee WK (ed) Pathology & genetics. Tumours of the nervous system. World Health Organization classification of tumours. IARC Press, Lyon, pp 29–39
Singh SK, Clarke ID, Terasaki M, Bonn VE, Hawkins C, Squire J, Dirks PB (2003) Identification of a cancer stem cell in human brain tumors. Cancer Res 63:5821–5828
Varlet P, Soni D, Miquel C, Roux FX, Meder JF, Chneiweiss H, Daumas-Duport C (2004) New variants of malignant glioneuronal tumors: a clinicopathological study of 40 cases. Neurosurgery 55:1377–1392
Watanabe K, Sato K, Biernat W, Tachibana O, von Ammon K, Ogata N, Yonekawa Y, Kleihues P, Ohgaki H (1997) Incidence and timing of p53 mutations during astrocytoma progression in patients with multiple biopsies. Clin Cancer Res 3:523–530
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shibahara, J., Fukayama, M. Secondary glioblastoma with advanced neuronal immunophenotype. Virchows Arch 447, 665–668 (2005). https://doi.org/10.1007/s00428-005-1263-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00428-005-1263-x