
Abstract
Purpose
To establish optimal management of patients with an umbilical hernia complicated by liver cirrhosis and ascites.
Methods
Patients with an umbilical hernia and liver cirrhosis and ascites were randomly assigned to receive either elective repair or conservative treatment. The primary endpoint was overall morbidity related to the umbilical hernia or its treatment after 24 months of follow-up. Secondary endpoints included the severity of these hernia-related complications, quality of life, and cumulative hernia recurrence rate.
Results
Thirty-four patients were included in the study. Sixteen patients were randomly assigned to elective repair and 18 to conservative treatment. After 24 months, 8 patients (50%) assigned to elective repair compared to 14 patients (77.8%) assigned to conservative treatment had a complication related to the umbilical hernia or its repair. A recurrent hernia was reported in 16.7% of patients who underwent repair. For the secondary endpoint, quality of life through the physical (PCS) and mental component score (MCS) showed no significant differences between groups at 12 months of follow-up (mean difference PCS 11.95, 95% CI − 0.87 to 24.77; MCS 10.04, 95% CI − 2.78 to 22.86).
Conclusion
This trial could not show a relevant difference in overall morbidity after 24 months of follow-up in favor of elective umbilical hernia repair, because of the limited number of patients included. However, elective repair of umbilical hernia in patients with liver cirrhosis and ascites appears feasible, nudging its implementation into daily practice further, particularly for patients experiencing complaints.
Trial registration
Clinicaltrials.gov, NCT01421550, on 23 August 2011.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Umbilical hernias are common in patients with liver cirrhosis and ascites, with an incidence of up to 20% [1, 2]. The presence of ascites increases the risk of developing an umbilical hernia, due to increased abdominal pressure. Weakening of the abdominal wall, muscle wasting when nutritional status is poor, and dilatation of the umbilical vein—enlarging the pre-existent fascial opening—in patients with portal hypertension are additional contributing factors [3, 4].
Currently, there are no guidelines for the management of an umbilical hernia and its timing of surgical repair in patients with liver cirrhosis and ascites. Traditional surgical dogma dictates not to perform umbilical hernia repair under these circumstances, because of the presumed high surgical risks and high recurrence rates after surgery [5, 6]. Additionally, portal hypertension is common in cirrhotic patients with ascites, and this requires special caution because a patent umbilical vein is often present. A reopened umbilical vein can be an important outflow for the portal circulation in patients with severe portal hypertension. In these patients, elective repair without liver transplantation has been reported to result in acute portal vein thrombosis due to ligation of the umbilical vein during hernia repair, which in turn causes subsequent liver failure, necessitating emergency liver transplantation [7].
However, refraining from umbilical hernia repair under these circumstances can also result in serious complications: incarceration or evisceration of the bowel could occur, followed by necrosis of the overlying skin, necessitating emergency surgery [4, 7, 8]. Even after liver transplantation, incarceration and strangulation can still occur in untreated umbilical hernias [8]. Moreover, several studies have shown that emergency surgery is generally associated with even higher risks of morbidity and mortality compared to elective surgery, particularly in patients with liver cirrhosis [6, 8,9,10,11,12]. This underlines that emergency surgery in this group of frail patients should be avoided and that elective umbilical hernia repair might be the most optimal management [13, 14]. Concordingly, several retrospective and prospective series have shown good results with elective umbilical hernia repair for patients with liver cirrhosis [8, 12, 14]. However, no randomized controlled trial on this matter has been performed. The aim of this study was to compare conservative treatment with the elective repair of umbilical hernia in patients with liver cirrhosis and ascites. We hypothesized that elective repair of the umbilical hernia would result in a significant reduction of the overall complication rate and a better quality of life compared to conservative treatment.
Methods
Study design
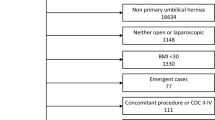
The CRUCIAL trial is a randomized controlled trial conducted in two centers. Patients with liver cirrhosis and ascites older than 18 years and a primary umbilical hernia were included in the study. The presence of ascites had to be proven on imaging or had to have been drained previously. Patients were randomized into one of two groups: patients in group 1 would undergo elective surgical repair and those in group 2 would receive conservative treatment. Irrespective of the randomization group, in the case of liver transplantation, patients would receive umbilical hernia repair simultaneously if the repair had not yet been performed. Excluded from participation were patients with a recurrent umbilical hernia following a midline laparotomy in the medical history, patients who presented with American Society of Anesthesiology (ASA) score IV or above, patients with incarcerated hernia requiring emergency repair, patients with a patent umbilical vein of more than 5 mm in diameter, and patients with an expected time to liver transplantation of less than 3 months.
The study protocol was approved by the institutional medical ethical review board of the Erasmus University Medical Center, Rotterdam, before the start of inclusion. All patients gave written informed consent. An independent data and safety monitoring board was constituted before the start of the trial, consisting of two independent surgeons and one biomedical statistician. All serious adverse events were reported to the institutional review board of the Erasmus University Medical Center. The progress of the trial and adverse events were reported to the safety monitoring board.
Randomization and masking
Patients were randomly allocated to either conservative treatment or elective repair by means of sealed, numbered envelopes that were opened in sequence. The randomization procedure was stratified for the participating center and for the model of end-stage liver disease (MELD) score ≤ 15 and > 15 and took place after collection of baseline information. Blinding for allocation did not take place for the participants, evaluators, and surgeons.
Procedures
All repairs (elective or during liver transplantation) took place using a (separate) infra-umbilical incision, dissection (avoiding resection) of the hernia sac, and restoration of the sac and its contents into the abdominal cavity. Intra-operative resection of the sac had to be recorded on the patient’s operation report. As mesh repair has been proven to reduce recurrence rates [15], non-absorbable monofilament sutures were combined with a flat circular polypropylene mesh placed in the onlay position or in the pre-peritoneal plane. The overlap of the mesh had to be at least 3 cm in each direction. Closure of the subcutaneous tissue and skin were performed at the discretion of the surgeon.
The preferred method of anesthesia was general anesthesia, allowing for local or spinal anesthesia in the case of contra-indications for general anesthesia. Antibiotic prophylaxis was administered 10 to 30 min preoperatively.
Patients were followed up at the outpatient clinic at 2 to 3 weeks, 3 months, 12 months, and 24 months after surgery. During these visits, patients underwent physical examination, and at the 12-month visit, they underwent abdominal ultrasonography to diagnose hernia recurrence. Quality of life measurements took place at baseline, 3, 6, 12, and 24 months through the Short Form-36 (SF-36) and the EuroQoL-5D (EQ-5D) questionnaire. The pain was evaluated through the visual analogue scale (VAS), anchored by “no pain” (score of 0), and “worst imaginable pain” (score of 100) on a 100-mm scale. To avoid clustering of scores around a preferred numeric value, numbers of verbal descriptors at intermediate points were not provided.
Outcomes
The primary outcome consisted of the hernia (and when applicable, its surgery)-related complications during 2 years of follow-up. Superficial or deep surgical site infection (SSI) [16], seroma, pneumonia, hematoma, urinary tract infection, and non-closure or delayed closure of the surgical wound at 4 weeks were considered minor complications. Major complications were mortality, evisceration, incarceration, necrosis of the overlying skin of the umbilical hernia, postoperative (> 2 weeks) leakage of ascites, liver failure, bacterial peritonitis, decompensated ascites, organ space SSI, or unexpected intensive care unit (ICU) admission related to the hernia or its repair.
These hernia-related complications were assessed for severity through the National Surgical Complication Registry (“Landelijke Heelkundige Complicatie Registratie” (LHCR)) grading tool (Table 1), scoring the maximal observed grade of hernia-related complications in each patient. Secondary endpoints were the cumulative hernia recurrence rate, pain, and quality of life.
Statistical analysis
The sample size was determined at 100 patients. This calculation was based on χ2 tests with α = 0.05, power of 90%, and an expected decrease in overall complication rate at 2 years from 50 to 15% due to elective repair of the umbilical hernia [8]. This requires 42 patients per treatment arm, 50 when accounting for a 20% loss to follow-up.
All patients were analyzed in the group randomized to (intention-to-treat). For the primary outcome—cumulative complication rate of the umbilical hernia in the two study arms—Kaplan-Meier curves were constructed and compared with the log-rank test. The maximal observed LHCR grade was compared with the χ2 test, and secondary outcomes were analyzed through linear mixed effect models, correcting for time, randomization group, gender, time to complication, and time to liver transplantation.
Statistical analysis was performed using R statistical software (version 3.3.1). This trial is registered at Clinicaltrials.gov; number NTC01421550.
Results
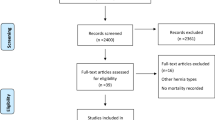
Due to unforeseen circumstances, the study was ended prematurely. Between February 2011 and July 2014, 34 patients were randomly assigned to either the intervention group (n = 16) or the conservative group (n = 18). Baseline characteristics are shown in Table 2. The median time of follow-up was 19.5 months (range 0 to 33.7 months).
Twenty-four-month morbidity
Eight patients (44.4%) in the conservative group received umbilical hernia repair: five received liver transplantation with simultaneous repair of the umbilical hernia, and three patients had elective or emergency repair due to complaints or incarceration. Of these eight patients, three developed recurrence of the umbilical hernia (16.7%). In the intervention group, only one patient had a recurrence of the umbilical hernia (6.3%). The mean length of stay after umbilical hernia repair was 3.21 days (range 1 to 9 days).
With regard to 24-month morbidity, 22 patients (64.7%) had at least one hernia-related complication, totaling 40 events. In the intervention group, eight patients (50%) experienced 18 events. In the wait-and-see group, 14 patients (78%) had 22 events.
In Table 3, the complications are split up for minor and major complications. Figure 1 is a Kaplan-Meier depiction of the time to first event per study arm. No difference between groups was found in time to the first event (p = 0.663). From Table 3, the difference in mortality between groups seems rather large, yet no statistical difference was found (p = 0.0682). The survival is also graphically depicted in Fig. 2. In the intervention group, one death occurred due to the development of spontaneous bacterial peritonitis resulting in multi-organ failure 1 week after surgery, the other death was due to the progression of end-stage malignant disease. In the wait-and-see group, mortality was due to subcapsular bleeding after the placement of a transjugular intrahepatic portosystemic shunt in one patient; the other causes were the progression of liver disease, end-stage malignant disease, and non-surgery-related pneumonia. Additionally, no statistical significance was observed between the LHCR grades in the two groups (p = 0.152).

Time to first complication. This complication can be either minor or major (including death). Censored patients are marked with “+”

Time to death. Censored patients are marked with “+”
When stratified for MELD score, more complications in total (n = 24 and n = 16, respectively) and more severe complications (n = 20 and n = 13, respectively) can be found in the group with patients having a score > 15, compared to the patient group with MELD score ≤ 15.
Secondary outcomes
With regard to the quality of life measured through the SF-36, the coefficients in the linear mixed model show that over time both the physical component score (PCS) and mental component score (MCS) increase for the intervention group, compared to a much smaller increase in the PCS and even a decrease in the MCS for the conservatively treated group (as shown by the negative coefficient for the interaction between the time and randomization group in Table 4). The model further reveals that liver transplantation causes patients to score higher on both component scores. Additionally, female patients appear to have a higher MCS than their male counterparts.
Quality of life measured through the EQ-5D questionnaire showed results similar to the SF-36 questionnaire. The created model showed that over time, quality of life increased (coefficient time 0.64, 95% CI 0.02–1.27). This increase was, however, smaller for the conservative group compared to the intervention group, shown by a negative coefficient (coefficient time:wait-and-see − 0.32, 95% CI − 1.33–0.69). Quality of life was at baseline already higher in the intervention group.
For pain outcomes, the coefficients in the created model show that pain decreases irrespective of the randomization group over time (coefficient time − 0.45, 95% CI − 0.99–0.09). At baseline, the scores were higher for women (coefficient 5.85, 95% CI − 12.59–24.29), and for patients in the wait-and-see group (coefficient wait-and-see 25.99, 95% CI 8.68–43.32).
Unfortunately, no cost-effectiveness analysis was performed due to the early termination of the study.
Discussion
In this study, equal numbers of hernia-related complications were observed for elective operation and conservative approach. Additionally, elective repair and wait-and-see treatment were associated with similar quality of life and pain scores. Though underpowered, this suggests that elective repair is safe in patients with liver cirrhosis and can be performed when the patient experiences complaints from his/her umbilical hernia.
In the current study, complication rates were high in both study arms. This is in line with expectations considering the high average MELD score observed in the patient group, as a higher MELD score is associated with higher perioperative morbidity and mortality in various types of elective procedures [17,18,19,20,21,22]. In the current study, patients with a MELD score ≥ 15 experienced more incarceration, skin necrosis, and unexpected ICU admission, and had a higher mortality rate. Despite the high numbers of complications, this study shows that even in patients with a relatively high MELD score, elective repair of the umbilical hernia is safe. Additionally, a conservative approach can also be accompanied by severe complications; our study showed more incarceration, decompensated cirrhosis, and ultimately death for the patients in the conservative treatment group than in the intervention group. Other authors describe a nearly 23% emergency surgery rate due to complications of a hernia during conservative treatment [23].
The most common cause of liver failure in our study was alcoholic liver cirrhosis. Alcoholic liver cirrhosis can cause large amounts of ascites [24], which is associated with complications, including umbilical hernia [25]. This association is applicable for both groups: a large amount of ascites can cause spontaneous bacterial peritonitis in both groups [26], more frequent incarceration and wound problems in the wait-and-see group [8, 27, 28], and more recurrence and postoperative leakage of ascites in the intervention group [28,29,30].
However, the results from our study need to be interpreted with caution. The major limitation of this study is the small patient group, due to the premature stop of the study. As a consequence, limited data were available for modeling the secondary outcomes, resulting in large confidence intervals. Especially at later time points, many patients had dropped out of the study due to death or other causes; this was however balanced between the two randomization groups.
Another consequence of the small patient group is the chance for clustering of confounders in the randomization process. This could have caused the difference already present at baseline for quality of life and VAS scores. However, these differences could also have been due to the fact that patients were not blinded for the randomization group they were in. The fact that patients knew they would receive an operation to relieve them of their umbilical hernia might have influenced how those patients filled out their quality of life forms. Nonetheless, the effect of the baseline differences on the secondary outcomes is more than marginal and necessitates careful consideration.
Despite the premature stop of patient inclusion, this study remains a methodologically well-performed randomized controlled trial, providing a higher level of evidence than small, retrospective cohorts with their inherent bias. Therefore—unfortunately not providing a definite answer to the management of umbilical hernias in patients with cirrhosis and ascites—this study is a valuable addition to the current body of knowledge on this subject and contributes to providing transparency to the scientific community. In the context of scientific integrity, this data can prove valuable in future meta-analyses, and refraining from reporting the data adds to the burden of publication bias.
Conclusion and implications
Despite not having enough power to show a significant difference between the two groups, this randomized controlled trial suggests that elective repair of an umbilical hernia does not cause excessive morbidity in cirrhotic patients—even with high MELD scores—and is thus advisable when the patient experiences complaints of the umbilical hernia. Considering this fact, one could argue that early elective repair when MELD scores are low—even in patients on the waiting list for transplantation—is the safer strategy. The definitive answer to whether elective umbilical hernia repair causes significantly less complications than watchful waiting in patients with liver cirrhosis remains unknown, which leaves room for further study.
Data availability
Not applicable
References
Chapman CB, Snell AM, Rowntree LG (1931) Decompensated portal cirrhosis: report of one hundred and twelve cases. JAMA. 97(4):237–244
Belghiti J, Durand F (1997) Abdominal wall hernias in the setting of cirrhosis. Semin Liver Dis 17(3):219–226
Shlomovitz E, Quan D, Etemad-Rezai R, McAlister VC (2005) Association of recanalization of the left umbilical vein with umbilical hernia in patients with liver disease. Liver Transpl 11(10):1298–1299
O’Hara ET, Oliai A, Patek AJ Jr, Nabseth DC (1975) Management of umbilical hernias associated with hepatic cirrhosis and ascites. Ann Surg 181(1):85–87
Leonetti JP, Aranha GV, Wilkinson WA, Stanley M, Greenlee HB (1984) Umbilical herniorrhaphy in cirrhotic patients. Arch Surg 119(4):442–445
Cho SW, Bhayani N, Newell P, Cassera MA, Hammill CW, Wolf RF, Hansen PD (2012) Umbilical hernia repair in patients with signs of portal hypertension: surgical outcome and predictors of mortality. Arch Surg 147(9):864–869
Reissfelder C, Radeleff B, Mehrabi A, Rahbari NN, Weitz J, Buchler MW et al (2009) Emergency liver transplantation after umbilical hernia repair: a case report. Transplant Proc 41(10):4428–4430
Marsman HA, Heisterkamp J, Halm JA, Tilanus HW, Metselaar HJ, Kazemier G (2007) Management in patients with liver cirrhosis and an umbilical hernia. Surgery. 142(3):372–375
Schumpelick V, Treutner KH, Arlt G (1994) Inguinal-Hernia Repair in Adults. Lancet. 344(8919):375–379
Primatesta P, Goldacre MJ (1996) Inguinal hernia repair: incidence of elective and emergency surgery, readmission and mortality. Int J Epidemiol 25(4):835–839
van den Heuvel B, Dwars BJ, Klassen DR, Bonjer HJ (2011) Is surgical repair of an asymptomatic groin hernia appropriate? A review. Hernia 15(3):251–259
de Goede B, Klitsie PJ, Lange JF, Metselaar HJ, Kazemier G (2012) Morbidity and mortality related to non-hepatic surgery in patients with liver cirrhosis: a systematic review. Best Pract Res Clin Gastroenterol 26(1):47–59
Belghiti J, Desgrandchamps F, Farges O, Fekete F (1990) Herniorrhaphy and concomitant peritoneovenous shunting in cirrhotic patients with umbilical hernia. World J Surg 14(2):242–246
Eker HH, van Ramshorst GH, de Goede B, Tilanus HW, Metselaar HJ, de Man RA, Lange JF, Kazemier G (2011) A prospective study on elective umbilical hernia repair in patients with liver cirrhosis and ascites. Surgery. 150(3):542–546
Kaufmann R, Halm JA, Eker HH, Klitsie PJ, Nieuwenhuizen J, van Geldere D, Simons MP, van der Harst E, van 't Riet M, van der Holt B, Kleinrensink GJ, Jeekel J, Lange JF (2018) Mesh versus suture repair of umbilical hernia in adults: a randomised, double-blind, controlled, multicentre trial. Lancet. 391(10123):860–869
Centers for Disease Control and Prevention (CDC) (2017) Guideline for the prevention of surgical site infection. [cited 2017 March 2]. Available from: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf.
Krafcik BM, Farber A, Eslami MH, Kalish JA, Rybin D, Doros G, Shah NK, Siracuse JJ (2016) The role of model for end-stage liver disease (MELD) score in predicting outcomes for lower extremity bypass. J Vasc Surg 64(1):124–130
Northup PG, Wanamaker RC, Lee VD, Adams RB, Berg CL (2005) Model for end-stage liver disease (MELD) predicts nontransplant surgical mortality in patients with cirrhosis. Ann Surg 242(2):244–251
Morimoto N, Okada K, Okita Y (2013) The model for end-stage liver disease (MELD) predicts early and late outcomes of cardiovascular operations in patients with liver cirrhosis. Ann Thorac Surg 96(5):1672–1678
Lau T, Ahmad J (2013) Clinical applications of the model for end-stage liver disease (MELD) in hepatic medicine. Hepat Med 5:1–10
Elnahas A, Nguyen GC, Okrainec A, Quereshy F, Jackson TD (2014) The effect of underlying liver disease on short-term outcomes following bariatric surgery. Surg Endosc 28(9):2708–2712
Lange EO, Jensen CC, Melton GB, Madoff RD, Kwaan MR (2015) Relationship between model for end-stage liver disease score and 30-day outcomes for patients undergoing elective colorectal resections: an American College of Surgeons-National Surgical Quality Improvement Program study. Dis Colon Rectum 58(5):494–501
Pinheiro RS, Andraus W, Waisberg DR, Nacif LS, Ducatti L, Rocha-Santos V et al (2020) Abdominal hernias in cirrhotic patients: surgery or conservative treatment? Results of a prospective cohort study in a high volume center: cohort study. Ann Med Surg (Lond) 49:9–13
Pedersen JS, Bendtsen F, Moller S (2015) Management of cirrhotic ascites. Ther Adv Chronic Dis 6(3):124–137
Huelin P, Fortea JI, Crepso J, Fábrega E (2017) Ascites: treatment, complications, and prognosis. In: Rodrigo L (ed) Ascites: physiopathology, treatment, complications and prognosis. IntechOpen
Kuiper JJ, van Buuren HR, de Man RA (2007) Ascites in cirrhosis: a review of management and complications. Neth J Med 65(8):283–288
Gray SH, Vick CC, Graham LA, Finan KR, Neumayer LA, Hawn MT (2008) Umbilical herniorrhapy in cirrhosis: improved outcomes with elective repair. J Gastrointest Surg 12(4):675–681
Coelho JC, Claus CM, Campos AC, Costa MA, Blum C (2016) Umbilical hernia in patients with liver cirrhosis: a surgical challenge. World J Gastrointest Surg 8(7):476–482
Rosemurgy AS, Statman RC, Murphy CG, Albrink MH, McAllister EW (1992) Postoperative ascitic leaks: the ongoing challenge. Surgery. 111(6):623–625
McKay A, Dixon E, Bathe O, Sutherland F (2009) Umbilical hernia repair in the presence of cirrhosis and ascites: results of a survey and review of the literature. Hernia. 13(5):461–468
Author information
Authors and Affiliations
Contributions
Study conception and design: De Goede, Lange, Metselaar, Kazemier; acquisition of data: De Goede, Van Kempen, Polak, De Man, Taimr, Lange, Metselaar, Kazemier; analysis and interpretation of data: van Rooijen; drafting of manuscript: van Rooijen, De Goede; critical revision: Van Kempen, Polak, De Man, Taimr, Lange, Metselaar, Kazemier.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
This study was approved by the Erasmus Medical Center research ethics committee and procedures adhered to the tenets of the Declaration of Helsinki.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
de Goede, B., van Rooijen, M.M.J., van Kempen, B.J.H. et al. Conservative treatment versus elective repair of umbilical hernia in patients with liver cirrhosis and ascites: results of a randomized controlled trial (CRUCIAL trial). Langenbecks Arch Surg 406, 219–225 (2021). https://doi.org/10.1007/s00423-020-02033-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-020-02033-4