
Abstract
Purpose
This study retrospectively compared different therapy modalities in patients with hepatocellular carcinoma (HCC) complicated by bile duct thrombi (BDT).
Methods
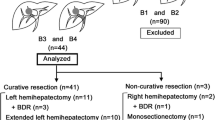
A total of 184 patients with BDT were selected from a pool of 12,114 patients with HCC, and their cases were reviewed in this study.
Results
The occurrence rate of BDT was 1.84% (223/12,114) in our study. The radical resection rate in types I, II, III, and IV was 70% (7/10), 38.46% (10/26), 20.4% (29/142), 33.3% (2/6), respectively. The mean survival time in patients who underwent radical hepatic resection and BDT removal (group A), palliative hepatectomy and BDT removal (group B), palliative hepatectomy and BDT removal plus unilateral liver artery ligation or postoperative transcatheter arterial chemoembolization (TACE; group C), TACE (group D), drainage to relieve the jaundice by ERCP or PTCD (group E), and conservative treatment (group F) was 37, 6, 16, 11, 3.0, 3.0 months, respectively. The survival rate of patients in group A was significantly greater than in other group (P < 0.0001); the rate in groups C and D was significantly higher than that in groups B, E, and F (P < 0.001). In group A, 1-year recurrence rate was 20.8% (10/48). One patient with severe jaundice suffered chronic liver failure after right lobe resection and died 2 months after operation. In groups B, C, D, E, and F, in ten cases, cholangitis occurred, in eight cases, hemobilia occurred, and 72 of 136 patients suffered liver failure and died within 6 months. Five patients underwent orthotopic liver transplantation; at the time of writing, three patients are still alive, and the longest survivor has now survived for 37 months since undergoing transplantation.
Conclusions
Radical hepatic resection and removal of BDT, combined with TACE, are the best approach for treating HCC patients with BDT. Biliary drainage to relieve the jaundice is critical.



Similar content being viewed by others


References
Ueda M, Takeuchi T, Takeyasu T et al (1994) Classification and Surgical treatment of hepatocellular carcinoma with bile duct thrombi. Hepatogastroenterology 41:349–354
Lau WY, Leung KL, Leung TWT et al (1997) A logical approach to hepatocellular carcinoma presenting with jaundice. Ann Surg 225:281–285. doi:10.1097/00000658-199703000-00007
Satoh S, Ikai I, Honda G et al (2000) Clinicopathologic evaluation of hepatocellar carcinoma with bile duct thrombi. Surgery 128:779–783. doi:10.1067/msy.2000.108659
Shiomi M, Junichi K, Nagino M et al (2001) Hepatocellular carcinoma with biliary tumor thrombi: Aggressive operative approach after appropriate preoperative management. Surgery 129:692–698. doi:10.1067/msy.2001.113889
Peng SY, Wang JW, Liu YB et al (2004) Surgical intervention for obstructive jaundice due to biliary tumor thrombus in hepatocellular carcinoma. World J Surg 28(1):43–46. doi:10.1007/s00268-003-7079-4
Fukuda S, Okuda K, Imamura M et al (2002) Surgical resection combined with chemotherapy for advanced hepatocellularcarcinoma with tumor thrombus: report of 19 cases. Surgery 131(3):300–310
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Xiangji, L., Weifeng, T., Bin, Y. et al. Surgery of hepatocellular carcinoma complicated with cancer thrombi in bile duct: efficacy for criteria for different therapy modalities. Langenbecks Arch Surg 394, 1033–1039 (2009). https://doi.org/10.1007/s00423-009-0496-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-009-0496-6