
Abstract
Purpose
To examine the influence of employment social support type (e.g. co-worker, supervisor, general support) on risk of occurrence of low back pain, and prognosis (e.g. recovery, return to work status) for those who have low back pain.
Methods
Systematic search of seven databases (MEDLINE, Embase, PsychINFO, CINAHL, IBSS, AMED and BNI) for prospective or case–control studies reporting findings on employment social support in populations with nonspecific back pain. Data extraction and quality assessment were carried out on included studies. A systematic critical synthesis was carried out on extracted data.
Results
Thirty-two articles were included that describe 46 findings on the effect of employment social support on risk of and prognosis of back pain. Findings show that there is no effect of co-worker, supervisor or general work support on risk of new onset back pain. Weak effects of employment support were found for recovery and return to work outcomes; greater levels of co-worker support and general work support were found to be associated with less time to recovery or return to work.
Conclusions
The evidence suggests that the association between employment support and prognosis may be subject to influence from wider concepts related to the employment context. This review discusses these wider issues and offers directions for future research.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Nonspecific low back pain (LBP) is very common. Two large population studies (Papageorgiou et al. 1995; Cote et al. 1998) place a lifetime prevalence of back pain at 60–80 %. This high prevalence has considerable impact within the employment sector. For example, in a study of back pain consulters from a UK primary care sample (Wynne-Jones et al. 2008), 37 % of those unemployed attributed this to their back pain, 22 % of those currently employed were on sickness absence and a further 11 % were on reduced duties at work due to their back pain. A recent report by the European Work Foundation ‘Fit for work’ (Bevan et al. 2009) reports that 25 % of workers in Europe suffer from back pain and estimate the total cost of musculoskeletal illness on employment productivity in Europe at €12 billion. This is further compounded by evidence that the longer a person is out of work due to back pain, the more difficult it is to re-engage into employment, and that recurrence rates are high (Waddell and Burton 2001).
In the light of the impact of back pain on employment, there has been a steady growth in interest in what employment factors impact on both risk for back pain and related outcomes such as sickness absence, recovery and return to work (Hartvigsen et al. 2004; Steenstra et al. 2005). One influential theoretical model, utilised within employment and illness research, is Karasek’s Demand Control Model (Karasek et al. 1998). According to the model having a job with high demands (e.g. high paced physical work), with no or little control over the decisions affecting work (e.g. fixed schedules, having a subordinate position), leads to an increase in stress and subsequent illness (Landsbergis et al. 2001). It is proposed that these outcomes can be modified if the person receives social support within the employment context (Johnson and Hall 1988; Theorell and Karasek 1996). This and similar theoretical models have been investigated within musculoskeletal research (Bongers et al. 2006) and have led to clinical guidelines on the consideration of work psychosocial factors (Costa-Black et al. 2010).
However, the evidence within systematic reviews on the impact of employment social support on back pain has been conflicting. The reasons given for inconsistency include difficulties synthesising evidence, due to variation in the measurement of work social support (Bongers et al. 2006; Hartvigsen et al. 2004; Steenstra et al. 2005; Woods 2005), and a lack of research focus specifically on work social support; for example, of the eight recent reviews (Bongers et al. 2006; Hartvigsen et al. 2004; Steenstra et al. 2005; Woods 2005; Waddell and Burton 2001; Hoogendoorn et al. 2000; Kuijer et al. 2006; Lakke et al. 2009), only one review (Woods 2005) solely considered work support issues using qualitative methodology.
The objective of this systematic review is to describe the evidence of employment-related social support on the risk of occurrence of a new episode of back pain and on the influence of employment-related support on prognosis once someone has back pain (e.g. recovery, return to work status). Furthermore, by way of a critical evidence synthesis, this review will address some current difficulties reported by previous reviews. This will be done by (1) stratification of evidence by study outcome (e.g. risk or prognosis), (2) stratification by type of support (e.g. co-worker, supervisor, general support), (3) critical assessment of the evidence based on the adequacy of the measure of employment social support and other key components of the included studies (e.g. response rate, attrition rate, geographic location, type of employment, sample size, sophistication of the analysis, length of follow up time, assessment of LBP).
Methods
This review uses a systematic approach to identify and synthesise research on employment social support (e.g. general level of support at work, level of supervisor support, level of co-worker support) within back pain populations.
Search strategy
The following computerised databases were searched from their respective inception dates up to 18 November 2011: MEDLINE, Embase, PsychINFO, CINAHL, IBSS, AMED and BNI. Reference lists of the studies and current relevant reviews were checked for additional study citations. Validated measures of social support were also citation checked using the ISI Web of Science citation mapping system, and databases of local experts were consulted for information on additional research studies.
Inclusion criteria
Articles were included if they had a focus on LBP populations (e.g. search term keywords: Back Pain, Low Back Pain), measured employment social support (e.g. search term keywords: Social Support, Social Interaction, Occupational Health Services, Employment Support, Employment Based Support), and provided data for the role of employment social support on risk of occurrence of LBP or prognosis with LBP outcomes such as pain intensity, disability or associated prognostic factors (search term keywords: Risk factors, Prospective, Epidemiologic Studies, Cohort studies, Case–Control Studies). The search terms (“Appendix 1”) were used as key words and also exploded to include all lower level headings (e.g. Mesh terms within MEDLINE).
Exclusion criteria
Studies were excluded that focused exclusively on family support or informal social support or included populations with other specific health problems (e.g. cancer, diabetes), studies solely on pregnant women, studies of surgical cohorts (e.g. lumbar fusion patients), studies of back pain patients who have a specific diagnosis (e.g. lumbar stenosis, spondylolithesis, spinal cord diseases, red flags). Cross-sectional findings were also excluded due to the inability to distinguish cause and effect, as were small case series studies due to being underpowered (e.g. studies of <30 people).
Procedure
Study abstracts were screened for clearly irrelevant studies, and for any study that was suitable, full text papers were obtained. Final selection of research papers was conducted by two reviewers (PC and KMD) using the inclusion and exclusion criteria.
Assessment of study biases
All included articles were subject to quality assessment of study methodology for bias; the studies’ focus on employment social support, the measurement of social support, study population, analysis undertaken, and the quality of reporting. Further assessments were carried out relating to the study design type, such as the attrition rate and follow-up period as additional criteria for cohort studies or screening of controls within a case–control study designs. It was not possible to use a pre-existing quality assessment tool due to the inclusion of differing study designs (e.g. cohort, case control) and inclusion of specific assessments (i.e. social support, back pain) so the quality assessment measure (“Appendix 2”) was based on the combination of assessments of a number of recent review articles and guidance on quality assessment within systematic reviews on the area of back pain (Woods 2005; Kuijer et al. 2006; Mallen et al. 2007; Hayden et al. 2009).
Articles were assessed using the quality assessment criteria checklist by two reviewers (PC, GWJ). Thereafter, all disagreements were discussed at a consensus meeting, and if disagreements were not resolved, a third reviewer (KMD) provided the final judgement.
Data extraction and synthesis
Study information on author, country, study population, sample size, response rate, follow-up period (cohort designs only), study design, focus, assessment of back pain, assessment of employment social support, analysis, outcome in relation to employment social support, findings and strength of reported effect were extracted from the studies. Full data extraction tables can be found in “Appendix 3”.
Analysis
Studies were grouped together corresponding to their respective study design, occurrence (e.g. risk of back pain) and prognosis (e.g. disability, return to work, sickness absence, recovery). Studies were also grouped to reflect the type of employment social support reported within the research papers (e.g. co-worker support, supervisor support, unspecified work support). Studies that did not describe the specific type of support (i.e. unspecified work support) are described as ‘General Work Support’ (GWS) within this review. In addition, some studies had multiple outcomes within the analysis (e.g. a prospective cohort study reports on incident risk and follows up on disability or a study that report’s findings both on co-worker support and supervisor support) and were included within the findings more than once.
Studies were then stratified dependent on whether or not they reported a significant association of employment support on risk outcome (i.e. risk of LBP) or prognosis (i.e. sickness absence, return to work status). The analysis centred on comparisons between studies that reported an association or not using key aspects of extracted data, measurement of social support (studies that used a measure that included multiple items to assess support type were judged as adequate, studies that used a single item or did not specify were judged as poor), geographic location (countries where studies were carried out), worker sample (e.g. industrial workers, office workers, general workers), analysis type (e.g. univariate, multivariate), assessment of back pain (e.g. pain intensity, disability, mechanical assessment, medical codes, prevalence and duration), factors of study bias (sample size, baseline response, attrition, length of follow-up).
Assessment of strength of association was carried out following criteria guidelines (Hartvigsen et al. 2004; Iles et al. 2008); individual study results are described as: none (e.g. non-significant result), weak (e.g. OR/RR 1.01–1.49), moderate (e.g. OR/RR 1.50–1.99) or strong (e.g. OR/RR ≥ 2.0) in the support of an association between employment social support and back pain outcomes.
Results
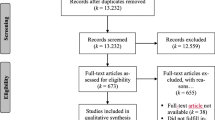
Systematic searching identified 375 publications (see Fig. 1). An additional 72 articles were included via alternative search strategies (hand search, expert consultation, and citation search). 378 articles were excluded following abstract screening (e.g. not nonspecific LBP population, duplicates) with a further 37 articles excluded following full text screening. The reasons for exclusion at the full text screening stage were studies solely focusing on family support, cross-sectional studies, studies on specific spinal pain populations (e.g. spondylolithesis, lumbar stenosis, spinal injury), or populations that focused on chronic pain patients outside of this study’s inclusion criteria (e.g. migraines, fibromyalgia, chronic widespread pain). This resulted in 32 suitable articles included within the review.

Flow diagram of review procedure
Quality assessment analysis
Taken together, all studies offered a clear research objective, 91 % described their recruitment procedure adequately, 69 % described the demographics of their study populations and 56 % reached a quality target criteria of a 70 % participation rate (see “Appendix 2” for quality assessment scores for each study). Most (81 %) of the studies employed a citable measure of employment social support. For cohort designs, only 48 % of studies reported their attrition rates or reported comparisons of responders and non-responders and over half of the cohort studies reported a higher than 20 % attrition rate. Table 1 outlines the findings of employment social support for risk and prognosis for the included studies.
Employment social support and risk of occurrence of back pain
In total, 20 studies report on 27 findings on the association of employment social support and occurrence of back pain. Of those findings, 20 reported no significant associations, one reported a strong reverse effect (a greater level of employment support increased the risk of back pain) and six reported an effect whereby lower levels of employment support increased the risk of back pain (Table 1). Of those six findings, three were judged as weak associations, one of moderate strength and two judged as strong effects.
Co-worker support (CWS)
Seven studies were included within this analysis, six of those studies reporting no effect (Andersen et al. 2007; Hoogendoorn et al. 2001; Ijzelenberg and Burdorf 2005; Kaila-Kangas et al. 2004; Krause et al. 1998; Rugulies and Krause 2005) and one study reporting a reverse effect of higher CWS increasing the risk of LBP (Kerr et al. 2001). Examination of the studies revealed that six utilised an adequate measure of employment support with one study using a measure judged as poor (Ijzelenberg and Burdorf 2005). Included studies covered a range of geographical areas, had a broad selection of employment type, and a broad range of assessments for back pain. All studies used multivariate statistical testing, report an average level of response to follow-up at 77 %, had a mean follow-up period of 7.6 years, and all included samples of 500 participants or over.
Supervisor support (SS)
Six studies were included within this analysis. Four studies reported no effect of SS on risk of LBP (Andersen et al. 2007; Hoogendoorn et al. 2001; Krause et al. 1998; Rugulies and Krause 2005) with two studies reporting a strong effect of lower levels of SS increasing the risk of LBP (Ijzelenberg and Burdorf 2005; Kaila-Kangas et al. 2004). Comparing studies that report no effect with those that do report an effect, all those reporting no effect were judged as having an adequate measure of SS, whereas one study reporting an effect (Ijzelenberg and Burdorf 2005) was judged as poor, using only a single question to assess support. Assessment of back pain was similar across all studies. Studies were also relatively similar on their geographic populations. All of the studies had sample sizes above 500. Average baseline response rates for studies reporting no effect was 75 % compared to 86 % for the Ijzelenberg and Burdorf (2005) study (Kaila-Kangas et al. 2004, failed to report a baseline response). Average attrition rates at follow-up for studies reporting no effect were 88 % compared to 57 % for the two studies that report an effect. However, this value of 57 % was markedly reduced by the Kaila-Kangas et al. (2004) study who report loss to follow-up at 33 % with the Ijzelenberg and Burdorf (2005) study reporting 86 %. The average follow-up time for studies that report no effect was 4.4 years in comparison with the studies that reported an effect were highly variable, with Ijzelenberg and Burdorf (2005) at 6 months and Kaila-Kangas et al. (2004) at 28 years.
General work support (GWS)
In total, 13 studies report on 14 findings for risk of back pain and GWS. Overall, 10 studies (Clays et al. 2007; Elfering et al. 2002; Fransen et al. 2002; Ghaffari et al. 2008; Gheldof et al. 2006; Gonge et al. 2002; Harkness et al. 2003; Josephson and Vingard 1998; Larsman and Hanse 2009; Shannon et al. 2001) report no effect and 4 show an effect, of those 3 show a weak effect (Clays et al. 2007; Feuerstein et al. 2001; Leino and Hanninen 1995) and 1 reports a moderate effect (Stevenson et al. 2001). Studies reporting no effect all included an adequate assessment of GWS, whereas two studies reporting an effect (Feuerstein et al., Stevenson et al.) were judged to have poor assessments. Assessment of pain was variable in studies that did not report an effect with measurements of back pain measured via compensation claim records, current pain, pain in the previous week, or pain in the previous 12 months. The assessment was less variable for studies reporting effects, all of them assessing pain within the previous 6–12 months. Geographic locations are similar for studies. Employment type was similar between studies reporting an effect and those who did not. Average sample sizes were found to be similar. There are differences in the average baseline response with an average of 67 % for studies reporting no effect compared to 44 % for those reporting an effect but average attrition rates are similar. All studies employed multivariable analysis. The average follow-up time was 2.3 years (3 months to 6 years) for studies reporting no effect compared to 6 years (2–10 years) for studies that do report an effect.
Employment social support and recovery from back pain
In total, 13 studies report 19 findings on the association between work support and return to work (RTW) for those with back pain. Overall, 11 findings report no association, 7 findings report associations whereby lower levels of work support delay RTW or recovery status and 1 study reports a weak reverse effect (Table 1). Of the findings of effect supporting an association between low work support and delays in RTW, 4 were judged as weak, 1 as moderate and 2 of strong effect.
Co-worker support (CWS)
In total, 4 studies report effects, 2 finding an association that lower levels of CWS delay RTW status (Mielenz et al. 2008; van den Heuvel et al. 2004), 1 reporting a reverse effect (Schultz et al. 2004) and 1 reporting no association (Helmhout et al. 2010). All studies were judged to have used an adequate measure of CWS. The assessment of LBP varied between studies: the study finding no association (Helmhout et al. 2010) using recurring LBP in the previous 4 weeks, the study reporting a reverse effect (Schultz et al.) measuring pain and disability in the previous 6 months, and the 2 studies reporting a positive association using biomechanical assessment (Mielenz et al. 2008) and presence of LBP in the previous 12 months (van den Heuvel et al. 2004). Geographic locations were similar for all studies. The 2 studies that report an association drew their samples from general workers, whereas the study reporting no association used a military sample, and the study reporting a reverse effect recruited general workers on current compensation for their LBP. Average sample size was larger for the studies reporting an association (1,042 vs. 190), and they also report a greater average response rate (88 vs. 32 %). Average follow-up response rates were lower for the 2 studies reporting an association (69 %) compared to 85 % for the Schultz et al. (2004) study; Helmhout et al. (2010) failed to report on attrition. Multivariable statistical testing was used by studies reporting an association, the study who reported no association and the study who found a reverse effect both used univariable analysis. Follow-up time was variable with the studies reporting a positive effect having the largest difference (8 weeks and 3 years), the study reporting no association at 6 months and the study reporting the reverse effect at 3 months.
Supervisor support (SS)
In total, 3 studies were included within this category. All studies reported no association between the level of SS and RTW status. All studies were judged to have adequate measures of SS, included a broad assessment of LBP, and covered a broad geographical area (Europe and USA). Multivariable testing was used by 2 studies (Mielenz et al. 2008; van den Heuvel et al. 2004). Length of follow-up was variable between studies with an average baseline response of 65 % and an average 68 % follow-up rate.
General work support (GWS)
For the effects of GWS on RTW status, 9 studies (Dionne et al. 2007; Gheldof et al. 2006; Heymans et al. 2006; Karlsson et al. 2010; Lotters and Burdorf 2006; Morken et al. 2003; Soucy et al. 2006; Tubach et al. 2002; van der Giezen et al. 2000) report on 12 findings. Of those findings, 5 are of an association between lower levels of GWS and delays in RTW status (4 of weak effect and 1 strong) and 7 findings of no association. All but one study that report no association (Lotters and Burdorf 2006), and all but one study that report an association (van der Giezen et al. 2000) included measures of GWS judged to be adequate. Assessment of LBP is variable within studies that report an association and those that do not, including current pain at time of assessment to pain within the previous 5 years, consultations and ICD coding. Geographic locations are generally similar between studies. Recruitment samples for studies that report associations are from general and industry workers, and also those involved in compensation claims; for studies reporting no association, there is recruitment from industrial workers but also those who have indicated working status from a random population sample, and health care consulters where work type was not recorded. Average sample sizes, baseline response rates, follow-up rates and follow-up time were similar for studies reporting no association and those reporting associations. All studies, except van der Giezen et al. (2000) who reported an association, used multivariable analysis.
Discussion
This review has carried out a systematic search for articles that reported on the effects of work social support on back pain from risk of occurrence and prognosis (recovery and return to work) studies. Overall, the evidence suggests no effect of work support as a risk factor for back pain; however, by examining the different types of support some distinctions occur. A similar picture emerges on the data and evidence for recovery and return to work with some evidence of CWS influencing outcome and mixed findings for GWS. The results suggest that employment-related support is less likely a factor on why someone gets back pain but could be an important factor on recovery and return to work once back pain is experienced.
Risk of occurrence of back pain
The evidence suggests that the level of support perceived from co-workers is not a factor in risk of back pain. For CWS, the included studies, all showing no or a reverse effect, incorporated an adequate range of measures on CWS, a broad range of employment types and a broad assessment of back pain. The results for the effects of SS do show some effect is present. However, the studies reporting effects had less adequate assessments of SS and highly variable follow-up periods (6 months and 28 years) and so the effect, although strong in both studies, has to be tempered with these differences. More research is needed to investigate whether SS is a risk factor for back pain. The results on risk and GWS show a similar pattern with no or little effect and no discernible differences on the key extracted data between studies that reported an effect and those that did not. One exception to this is the lesser variability on the assessment of pain in studies reporting an effect (presence of back pain in the previous 6–12 months). This may have led to an inflated incidence rate compared to perhaps more stringent assessments of compensation claims or current pain used in some of the studies reporting no effect. However, notably three studies that reported no effect (Gheldof et al. 2006; Josephson and Vingard 1998; Larsman and Hanse 2009) could be considered as non-significant trends and so more information is needed before conclusions can be drawn.
Prognosis for back pain
Overall, the evidence for prognosis is less clear with mixed findings for both CWS and GWS. The results for CWS, considering the key elements of study bias, suggest that the findings of an effect (less CWS delays recovery and return to work status) are more robust than those reporting no effect or a reverse effect. It may be that a supportive co-worker environment is important for those who have back pain, and this study’s finding supports the finding of a previous review (Steenstra et al. 2005), who showed a small pooled effect of CWS and work-related prognostic outcomes for those with back pain. The results for SS show no effect for all the included studies. This suggests that the perception of support directly from supervisors is not a factor in recovery. However, due to only three included studies, more research is needed. Findings are mixed for evidence of an effect of GWS on recovery and return to work with no apparent differences in key areas of bias between studies reporting and not reporting an effect. A reason for the stronger presence of an effect for GWS compared to SS could be that the measure of GWS is more than just a measure of support per se. For example, many of the studies that have measured general work support have included within their support measures aspects such as: perceived satisfaction of support (Leino and Hanninen 1995; Fransen et al. 2002), emotional aspects of support (Elfering et al. 2002), questions on work output (Fransen et al. 2002), conflict within the employment context (Larsman and Hanse 2009) or have used generic unspecified measures of support (Gonge et al. 2002; Ghaffari et al. 2008; Shannon et al. 2001;Morken et al. 2003; van der Giezen et al. 2000; Heymans et al. 2006). These aspects could be seen as support items but also as part of a larger concept of the workers’ general evaluation of their job. According to Karasek et al. (1998), aspects such as satisfaction with work, level of demands on the worker, the level of control the worker has, level of conflict at work are all important in their own right. It may be that the measures of general work support have been influenced by some of these factors. This therefore suggests that aspects involved in the supportive context for workers are important as prognostic factors for back pain; however, due to the variation in measurements used by studies in this review, the exact constructs relating to this are indistinct.
Taken together, the results for risk and prognosis show a weak effect of employment-related support for those with back pain. Less clear are the mechanisms that explain this association and this may be partly due to the ambiguity on what is meant by ‘support’ in an employment context. For example, a recent review by Woods (2005) included aspects of support such as satisfaction with employment, emotional support, conflict in the workplace, policy on occupational health, level of communication, health and safety policy, sickness absence policy, whereas other reviews such as Hartvigsen et al. (2004) have only reported on effects of direct co-worker support and supervisor support; Steenstra et al. (2005) and Hoogendoorn et al. (2001) have both included measures of problematic relations with other workers, whereas Kuijer et al. (2006) did not clearly specify what they meant by employment social support. This then broadens the scope of the concept of ‘support’ and this variation in definition may have contributed to the level of inconsistency described in previous reviews. Interestingly, this review could be construed as spanning this inconsistency, with no or very weak evidence of an effect for specific measures of CWS and SS (e.g. similar to Harvigsen et al.) but an increase in association for the generic GWS concept (e.g. similar to Woods). Many of the studies within the review who report GWS have combined measures of CWS and SS, and it is suggestive that some effect is there but it appears greater than the sum of its parts. Future research needs to consider the inherent complexity in the conceptualisation of employment social support (for a fuller explanation see “Appendix 4”). Furthermore, as mentioned in the introduction, the concept of employment co-worker and supervisor support forms only part of a larger model proposed by Karasek et al. (1998). There is a need to consider the component influence of employment social support as a moderator by using more sophisticated statistical modelling (e.g. path analysis, structural equation modelling) if we are to understand the role of employment social support, and in what context, on outcomes of spinal pain. Added to this is the evidence of the heterogeneity in the measurement of the outcome of back pain within this review. Studies differed in their assessment (patient rated, biomechanical testing, compensation status, different time scales for assessment) which makes comparisons all the more complex; future reviews should consider this issue.
Comparison with other reviews
This review has concentrated on the effects of employment social support, whereas most other reviews have considered this as part of a wider search of employment psychosocial factors. This has led other reviews to include only a small number of studies on which to base their conclusions, for example, Steenstra et al. (2005) based theirs on four studies, Hoogendoorn et al. (2000) on six studies and Hartvigsen et al. (2004) on nine studies. The greater number of studies included in this review (thirty-two) has enabled a more specified focus on employment support type and outcome (risk and prognosis), which we believe has overcome some of the issues of heterogeneity and inconsistency described by previous reviews.
Strengths and limitations
While this review has a comprehensive systematic search strategy, it did not include studies in languages other than English and so may have missed important findings; however, we did include studies from a range of countries worldwide. In addition, no review is completely immune from publication bias, and it may be the case that there are other findings (grey literature) we have not accessed. Strengths of the study are: the use of a systematic critical synthesis of the evidence which has enabled a closer inspection of the term employment social support and a better assessment of the types of support combined with an examination of individual study bias on the associations.
Further research
This review has highlighted a need for consensus on what is meant by the term ‘employment social support’. As mentioned previously, there are a number of differing conceptualisations and future research needs to report on those concepts to facilitate easier comparisons for future reviews but also, more importantly, to understand what factors of employment social support associate with outcomes. Secondly, and related to the first point, there is a need for research to consider the role of theoretical models within their research. Many studies (over 50 % in this review) employed the Karasek Job Content Questionnaire, or a derivative, as their measure of employment social support. However, studies did not perform the appropriate analysis techniques to ascertain whether employment social support is a moderator component as prescribed by the Karasek model.
Conclusion
This review has shown that employment-related support has little to no effect on risk of occurrence but a more notable effect on prognosis for those with back pain. The overall effect is weak for these findings; however, a greater understanding of the construct of ‘support’ in an employment context, and what factors interact with support, may lead to important pathways to reduce risk and reduce sickness absence, which could then be implemented by employers and occupational health practitioners.
References
Andersen JH, Haahr JP, Frost P (2007) Risk factors for more severe regional musculoskeletal symptoms: a two-year prospective study of a general working population. Arthritis Rheum 56(4):1355–1364
Bevan S, Quadrello T, McGee R, Mahdon M, Vavrosky A, Barham L (2009) Fit for work? Musculoskeletal disorders in the European workforce 1:1–143. The Work Foundation
Bigos SJ, Battie MC, Spengler DM, Fisher LD, Fordyce WE, Hansson TH, Nachemson AL, Wortley MD (1991) Prospective study of work perceptions and psychosocial factors affecting the report of back injury. Spine 16(1):1–6
Bongers PM, Ijmker S, van den Heuvel S, Blatter BM (2006) Epidemiology of work related neck and upper limb problems: psychosocial and personal risk factors (Part I) and effective interventions from a bio behavioural perspective (Part II). J Occup Rehab 16(3):279–302
Chronister JA, Johnson EK, Berven NL (2006) Measuring social support in for back pain patients: do patients care who provides what? J Behav Rehabil Disabil Rehabil 28(2):75–84
Clays E, De BD, Leynen F, Kornitzer M, Kittel F, De BG (2007) The impact of psychosocial factors on low back pain: longitudinal results from the belstress study. Spine 32(2):262–268
Costa-Black KM, Loisel P, Anema JR, Pransky G (2010) Back pain and work. Best Pract Res Clin Rheumatol 24(2):227–240
Cote P, Cassidy JD, Carroll L (1998) The Saskatchewan Health and Back Pain Survey. The prevalence of neck pain and related disability in Saskatchewan adults. Spine 23(15):1689–1698
Dionne CE, Bourbonais R, Fremont P, Rossignol M, Stock SR, Nouwen A, Larocque I, Demers E (2007) Determinants of “return to work in good health” among workers with back pain who consult in primary care settings: a two year prospective study. Eur J Spine 16:641–655
Elfering A, Semmer NK, Schade V, Grund S, Boos N (2002) Supportive colleague, unsupportive supervisor: the role of provider-specific constellations of social support at work in the development of low back pain. J Occup Health Psychol 7(2):130–140
Feuerstein M, Berkowitz SM, Haufler AJ, Lopez MS, Huang GD (2001) Working with low back pain: workplace and individual psychosocial determinants of limited duty and lost time. Am J Ind Med 40(6):627–638
Fransen M, Woodward M, Norton R, Coggan C, Dawe M, Sheridan N (2002) Risk factors associated with the transition from acute to chronic occupational back pain. Spine 27(1):92–98
Ghaffari M, Alipour A, Farshad AA, Jensen I, Josephson M, Vingard E (2008) Effect of psychosocial factors on low back pain in industrial workers. Occup Med 58(5):341–347
Gheldof EL, Vinck J, van den BE, Vlaeyen JW, Hidding A, Crombez G (2006) Pain and pain-related fear are associated with functional and social disability in an occupational setting: evidence of mediation by pain-related fear. Eur J Pain 10 (6):513–525
Gonge H, Jensen LD, Bonde JP (2002) Are psychosocial factors associated with low-back pain among nursing personnel? Work Stress 16(1):79–87
Harkness EF, Macfarlane GJ, Nahit ES, Silman AJ, McBeth J (2003) Risk factors for new onset low back pain amongst cohorts of newly employed workers. Rheumatology 42:959–968
Hartvigsen J, Lings S, Leboeuf-Yde C, Bakketeig L (2004) Psychosocial factors at work in relation to low back pain and consequences of low back pain; a systematic, critical review of prospective cohort studies. Occup Environ Med 61(1):e2
Hayden JA, Chou R, Hogg-Johnson S, Bombardier C (2009) Systematic reviews of low back pain prognosis had variable methods and results: guidance for future prognosis reviews. J Clin Epidemiol 62(8):781–796
Helmhout PH, Staal JB, Heymans MW, Harts CC, Hendriks EJ, de Bie RA (2010) Prognostic factors for perceived recovery or functional improvement in non-specific low back pain: secondary analyses of three randomized clinical trials. Eur Spine J 19(4):650–659
Heymans MW, de Vet HC, Knol DL, Bongers PM, Koes BW, van MW (2006) Workers’ beliefs and expectations affect return to work over 12 months. J Occup Rehabil 16 (4):685–695
Hoogendoorn WE, van Poppel MN, Bongers PM, Koes BW, Bouter LM (2000) Systematic review of psychosocial factors at work and private life as risk factors for back pain. Spine 25(16):2114–2125
Hoogendoorn WE, Bongers PM, de Vet HCW, Houtman ILD, Ariens GAM, van Mechelen W, Bouter LM (2001) Psychosocial work characteristics and psychological strain in relation to low-back pain. Scand J Work Environ Health 27(4):258–267
Ijzelenberg W, Burdorf A (2005) Risk factors for musculoskeletal symptoms and ensuing health care use and sick leave. Spine 30(13):1550–1556
Iles RA, Davidson M, Taylor NF (2008) Psychosocial predictors of failure to return to work in non-chronic non-specific low back pain: a systematic review. Occup Environ Med 65(8):507–517
Johnson JV, Hall EM (1988) Job strain, work place social support, and cardiovascular disease: a cross sectional study of a random sample of the Swedish working population. Am J Public Health 78:1336–1342
Josephson M, Vingard E (1998) Workplace factors and care seeking for low-back pain among female nursing personnel. Scand J Work Environ Health 24(6):465–472
Kaila-Kangas L, Kivimaki M, Riihimaki H, Luukkonen R, Kirjonen J, Leino-Arjas P (2004) Psychosocial factors at work as predictors of hospitalization for back disorders. Spine 29(16):1830–1832
Karasek R, Brisson C, Kawakami N, Houtman I, Bongers P, Amick B (1998) The Job Content Questionnaire (JCQ): an instrument for internationally comparative assessments of psychosocial job characteristics. J Occup Health Psychol 3(4):322–355
Karlsson N, Skargrin E, Kristenson M (2010) Emotional support predicts more sickness absence and poorer self assessed work ability: a two year prospective cohort study. BMC Public Health 10:648
Kerr MS, Frank JW, Shannon HS, Norman RW, Wells RP, Neumann WP, Bombardier C (2001) Biomechanical and psychosocial risk factors for low back pain at work. Am J Public Health 91(7):1069–1075
Krause N, Ragland DR, Fisher JM, Syme SL (1998) Psychosocial job factors, physical workload, and incidence of work-related spinal injury: a 5-year prospective study of urban transit operators. Spine 23(23):2507–2516
Kuijer W, Groothoff JW, Brouwer S, Geertzen JH, Dijkstra PU (2006) Prediction of sickness absence in patients with chronic low back pain: a systematic review. J Occup Rehabil 16(3):439–467
Lakke SE, Soer R, Takken T, Reneman MF (2009) Risk and prognostic factors for non-specific musculoskeletal pain: a synthesis of evidence from systematic reviews classified into ICF dimensions. Pain 147(1–3):153–164
Landsbergis PA, Schnall PL, Belkic KL, Baker D, Schwartz J, Pickering TG (2001) Work stressors and cardiovascular disease. Work 17(3):191–208
Larsman P, Hanse JJ (2009) The impact of decision latitude, psychological load and social support at work on the development of neck, shoulder and low back symptoms among female human service organization workers. Int J Ind Ergon 39:442–446
Leino PI, Hanninen V (1995) Psychosocial factors at work in relation to back and limb disorders. Scand J Work Environ Health 21(2):134–142
Lotters F, Burdorf A (2006) Prognostic factors for duration of sickness absence due to musculoskeletal disorders. Clin J Pain 22:212–221
Mallen CD, Peat G, Thomas E, Dunn KM, Croft PR (2007) Prognostic factors for musculoskeletal pain in primary care: a systematic review. Br J Gen Pract 57(541):655–661
Masters KS, Stillman AM, Spielmans GI (2007) Specificity of social support. Medicine 30(1):11–20
Mielenz TJ, Garrett JM, Carey TS (2008) Association of psychosocial work characteristics with low back pain outcomes. Spine 33(11):1270–1275
Morken T, Riise T, Moen B, Hauge SHV, Holien S, Langedrag A, Pedersen S, Saue ILL, Seljebo GM, Thoppil V (2003) Low back pain and widespread pain predict sickness absence among industrial workers. BMC Musculoskelet Disord 4:1–8
Papageorgiou AC, Croft PR, Ferry S, Jayson MI, Silman AJ (1995) Estimating the prevalence of low back pain in the general population. Evidence from the South Manchester Back Pain Survey. Spine 20 (17):1889–1894
Rugulies R, Krause N (2005) Job strain, iso-strain, and the incidence of low back and neck injuries. A 7.5-year prospective study of San Francisco transit operators. Soc Sci Med 61(1):27–39
Schultz IZ, Crook J, Meloche GR, Berkowitz J, Milner R, Zuberbier OA, Meloche W (2004) Psychosocial factors predictive of occupational low back disability: towards development of a return-to-work model. Pain 107(1–2):77–85
Shannon HS, Woodward CA, Cunningham CE, McIntosh J, Lendrum B, Brown J, Rosenbloom D (2001) Changes in general health and musculoskeletal outcomes in the workforce of a hospital undergoing rapid change: a longitudinal study. J Occup Health Psychol 6(1):3–14
Soucy I, Truchon M, Cote D (2006) Work-related factors contributing to chronic disability in low back pain. Work 26(3):313–326
Steenstra IA, Verbeek JH, Heymans MW, Bongers PM (2005) Prognostic factors for duration of sick leave in patients sick listed with acute low back pain: a systematic review of the literature. Occup Environ Med 62(12):851–860
Stevenson JM, Weber CL, Smith JT, Dumas GA, Albert WJ (2001) A longitudinal study of the development of low back pain in an industrial population. Spine 26(12):1370–1377
Theorell T, Karasek RA (1996) Current issues relating to psychosocial job strain and cardiovascular disease research. J Occup Health Psychol 1(1):9–26
Tubach F, Leclerc A, Landre MF, Pietri-Taleb F (2002) Risk factors for sick leave due to low back pain: a prospective study. J Occup Environ Med 44(5):451–458
van den Heuvel SG, Ariens GAM, Boshuizen HC, Hoogendoorn WE, Bongers PM (2004) Prognostic factors related to recurrent low-back pain and sickness absence. Scand J Work Environ Health 30(6):459–467
van der Giezen AM, Bouter LM, Nijhuis FJ (2000) Prediction of return-to-work of low back pain patients sicklisted for 3–4 months. Pain 87(3):285–294
Waddell G, Burton AK (2001) Occupational health guidelines for the management of low back pain at work: evidence review. Occup Med (Lond) 51(2):124–135
Woods V (2005) Work-related musculoskeletal health and social support. Occup Med (Lond) 55(3):177–189
Wynne-Jones G, Dunn KM, Main CJ (2008) The impact of low back pain on work: a study in primary care consulters. Eur J Pain 12(2):180–188
Acknowledgments
Systematic review advice from Jo Jordan and Danielle van der Windt both from the Arthritis Research UK Primary Care Centre, Keele University. This work was supported by the Wellcome Trust [083572].
Conflict of interest
All authors state no conflicts of interest.
Open Access
This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix 1
See Table 2.
Appendix 2
See Table 3.
Appendix 3
See Table 4.
Appendix 4: Assessment of employment social support
As evidenced from this review the assessment of employment support is multifaceted. Initially Johnson and Hall (1988) introduced the concept of work social support in the context of Karasek’s (1981) ‘Demand Control Model’ of job strain and illness outcomes. They showed that the level of social interaction between workers modified the association between job strain and cerebrovascular disease. Initial conceptualisation and measurement was restricted to a measure of the social interaction between workers with measurement of the level of communication between workers in times of work breaks, and as part of their working day in addition to the social interaction between workers outside of the employment context. Karasek et al. (1998) added to this concept by assessing the level of emotional support from both co-workers and supervisors as well as assessing the level of instrumental support (i.e. getting assistance to get their job done). The majority of the studies included within this review have based their assessment on the Karasek model, or the Work Apgar measure (Bigos et al. 1991); both of which primarily assess relationships between the worker and co-worker or supervisor, as well as the general work atmosphere. However Woods’ (2005) qualitative review acknowledged that other aspects of support may be equally important and included additional concepts such as; acceptance by peers at work, structural support (i.e. health and safety policy, management of occupational health), health specific (i.e. the ability to discuss health issues with employers), work and personal issues (the ability to discuss issues with employers both about work and personal), level of satisfaction, level of conflict and hostility within work, working alone and feeling isolated, social support outside of the work context.
This additional level of complexity is reflected within research on social support in general. Chronister et al. (2006) discusses the issue on the assessment of general social support and conceptualises the contingencies for social support on a number of differing levels. The first level is the structure; network (who offers the support), size (what size is the network, how many people), frequency (how frequent is the support available). The second level is support type; instrumental (actual practical support given by others), emotional (ability to discuss emotional issues), advice (having the availability to source advice specific to the issues the person faces), appraisal/affirmation (being affirmed and acknowledged by others). The third level is the perception of the support; it may be that all these levels of support are in place but the perception by the person will still be key as to whether the support is seen as helpful. For example, a study by Masters et al. (2007) considered social support within a health context and showed that social support can be perceived differently dependent on who is giving the support, over and above having the availability of the support.
The above evidence illustrates the complexity inherent when assessing employment social support. Future research of employment support needs to acknowledge and accommodate the complexity if we are to assess the estimates of the effect of employment social support on the outcomes for those with back pain.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Campbell, P., Wynne-Jones, G., Muller, S. et al. The influence of employment social support for risk and prognosis in nonspecific back pain: a systematic review and critical synthesis. Int Arch Occup Environ Health 86, 119–137 (2013). https://doi.org/10.1007/s00420-012-0804-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-012-0804-2