
Abstract
Objective
There is no information on the duration of absence of depressed Dutch workers. The aim of this study was to determine the duration of sickness absence due to depressive symptoms in the working population.
Methods
In this observational study of 15% of the Dutch working population, all absence episodes (n = 9,910) starting between April 2002 and November 2005 diagnosed as depression were selected. For these episodes, Kaplan–Meier survival curves were computed.
Results
The mean (and median) duration of sickness absence due to depressive symptoms was 200 (179) days in men and 213 (201) days in women. In both sexes, older employees had longer absence durations. Depressive symptoms had an estimated rate of chronicity (1 year of absence) of 24%. Employees in educational and public services (232 days in men and 242 days in women), commercial services (213 days in men and 219 days in women) and health care (212 days in men and 214 days in women) had the longest mean duration of absence with depressive symptoms. Men in the industrial sector (189 days) had the shortest absence periods. Employees in large sized companies (188 days in men and 208 days in women) had shorter absence episodes as compared to companies with less than 75 employees (214 days in men and 226 days in women).
Conclusions
Workers with depressive symptoms were absent for a long time. Explanations for the long duration are discussed. It is recommended to develop and apply tools for recognizing employees at risk for chronic depression.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Mental illness is an important cause of disability and its impact on job performance and productivity is substantial. Depression is one of the most common mental disorders. According to the World Health Organization (2002), depression will be the leading cause of morbidity by the year 2010. Depression was found to be related to long absence from work (Harrison and Martocchio 1998; Nieuwenhuijsen et al. 2006) and to be a significant predictor of work disability (Kouzis and Eaton 1994; Skodol et al. 1994; Kessler et al. 1999). Depressed employees had a 28 times higher risk of absence as compared to employees who did not suffer from depression (Kouzis and Eaton 1994). Respondents with depression reported a mean of 35 days (95% CI 27–44) in the past year when they were totally unable to work or carry out their normal activities because of their depression (Kessler et al. 2003). When depressed employees stayed at work, they had a lower than normal productivity (Kessler and Frank 1997).
Depressive episodes were reported to vary widely in their duration, with a median ranging from 2 to 12 months and with rates of chronicity (i.e. a duration of 12 months or more) between 15% and 50% (Keller et al. 1982; Coryell et al. 1994; Mueller et al. 1996; Eaton et al. 1997; Solomon et al. 1997; Spijker et al. 2002; Furukawa et al. 2005). Estimates of the mean duration of depressive episodes varied from 13 to 27 weeks (Blazer et al. 1994; Eaton et al. 1997; Kendler et al. 1997; Kessler et al. 2003).
In international research the duration of sickness absence due to depressive disorder was 142 days in 213 adult psychiatric outpatients (Sorvaniemi et al. 2003). In Norway, the mean sickness absence duration in psychiatric patients amounted to 110 days in men and 103 days in women (median 57 and 52 days, respectively), with depression as the most common diagnosis (Hensing et al. 2000). In a Swedish sick-leave database a mean sickness absence duration due to combined depression and anxiety disorders was 73 days in men and 75 days in women (Hensing et al. 1996). In a reference population consisting of working people, the mean duration of a major depression was 52 days for a single episode (with 4.1% lasting longer than 6 months) and 74 days for a recurrent episode (with 9.2% lasting longer than 6 months) according to the Medical Disability Advisor (2006). There is no information on the duration of absence of depressed workers in The Netherlands (Raddjoe and van der Hoek 2005). The results of international studies are not comparable to the Dutch situation, because of differences in social legislation and sickness absence regulations.
As it is very likely that the results of international studies are not comparable to the Dutch situation, the aims of this study were: (a) to investigate the mean (and median) duration of absenteeism due to depressive symptoms in the Dutch working population by sector and company size, and (b) to investigate gender and age influences on the mean (median) duration of absenteeism due to depressive symptoms.
Studies on sickness absence because of depression revealed gender differences, with men having a higher risk of sickness absence when depressed (Laitinen-Krispijn and Bijl 2000). Women had a higher incidence of sickness absence due to mental illness (North et al. 1993; Hensing et al. 1996, 2000), but the duration of sick-leave spells due to mental illness were longer for men (Hensing et al. 1996, 2000). Based on Dutch national statistics (Central Statistical Office of the Netherlands 2006), in which women have longer absence durations and higher disability figures than men, we hypothesize that depressed women have longer absence durations than men (H1). We also hypothesize that older employees have longer absence durations than younger employees (H2) based on Dutch national statistics and studies of Hensing et al. (1996, 2000). Furthermore, we hypothesize that employees in small companies have longer absence durations as compared to employees in large companies (H3), because of less reintegration opportunities in small companies. Finally, we hypothesize that employees in educational and health care services have longer absence durations as compared to employees in other sectors (H4). Employees in the education and care sectors have a substantially increased risk of being at work when sick, because of difficulties in replacement (Aronsson et al. 2000) and therefore, when they take absence the duration may be longer.
Methods
Data
The prevention, supervision and medical examination of sickness absence is a task of the employer for which he can choose to engage an occupational health department. ArboNed (the second largest occupational health department in the Netherlands) employs an absenteeism registration system for their affiliated companies. We register sickness absence and its causes in about 15% of the total Dutch working population. In our population, commercial services are over-represented (57% vs. 41%) and non-commercial services (e.g. health care, civil servants) are under-represented (17% vs. 34%) as compared to the total working population in the Netherlands.
All absence periods that started between April 2002 and November 2005, and were diagnosed as depression were selected from the registration system. Absence periods were encoded as depression by the occupational physician when symptoms of depressed mood (such as feelings of profound sadness or emptiness) and/or reduced interest in activities that used to be enjoyed lasted for at least two weeks in combination with 3 or more of the following symptoms: decreased energy, decreased motivation, appetite changes, disturbed sleep pattern, agitation or inhibition, guilt feelings, low sense of self-worth, impaired concentration, or self-destructive thoughts. The symptoms must be accompanied by evident suffering and adverse effects on personal as well as social functioning.
The age of the employees was registered at the moment of sick-leave. Absent men had a mean age of 41.6 years (SD = 9.9) and women of 38.2 years (SD = 9.9) (T = 17.2; df = 9,864; P < 0.01). The company size in which the employee worked was divided into four categories: <75 employees, 75–500 employees, 500–5,000 employees and >5,000 employees. In 95% of cases the company size was known. The companies were categorized into the following sectors (mean age ± standard deviation): construction industry (40.2 ± 10.2), health care (39.6 ± 10.1), trade (38.1 ± 10.3), catering industry (37.5 ± 10.0), industry (40.9 ± 9.8), education and public sector (43.9 ± 9.9), transportation and communication (41.0 ± 9.7), commercial services (38.6 ± 9.9), Other/unknown (39.9 ± 9.9). In 72% of cases the sector was known.
Absence duration
Between April 2002 and November 2005 a total of 9,910 newly originating episodes of absence due to depressive symptoms were registered. The period (in calendar days) between the first day of sick-leave and the date of return to work or disability pension was computed. In The Netherlands an employee can benefit a disability pension after one year of work incapacityFootnote 1. Absence periods of 365 or more calendar days were considered to reach this limit, and therefore the maximal duration of an absence episode was 365 days.
Absence duration was not corrected for part-time return to work, unless mentioned otherwise. When the number of absence days is corrected for part-time return to work, this is done by dividing the number of absence days by 1/reintegration percentage. For example, when the employee returns to work for 50% the number of absence days is divided by 2.
When estimating the duration of absence spells, it is important to censor absences which have not ended by the end of the observation period or at the dismissal date (Blossfeld and Rohwer 2002). Therefore, we censored absences that did not end before the retrieval date (November 1, 2005). Absences which ended, because the employee resigned, were also censored.
Statistical methods
The data were analyzed using SPSS for Windows, version 13. Kaplan–Meier survival curves were computed in order to obtain mean and median absence duration. The Kaplan–Meier method (Kaplan and Meier 1958) calculates the risk set at every point in time where at least one recovery occurred. The risk set also includes episodes that are censored at this point in time. A censored episode contains the information that there was no return to work or reaching the one-year absence limit at the end of the study period or the dismissal date. The survival functions were plotted using life tables. The mean number of absence days corrected for part-time return to work in the different groups was compared using analysis of variance.
If the main effect was significant, the Tukey post hoc test was performed in order to determine which groups differed from each other.
Results
In the period April 2002 to November 2005, 9,540 employees were absent with depressive symptoms. This is about 1% of the population covered by the occupational health department. Of these employees 9,196 (96.4%) had one absence episode, 321 (3.4%) had two absence episodes and 23 (0.2%) had three or more episodes of absence due to depressive symptoms. In Table 1, the course of sick-leaves with depressive symptoms is presented. Men more often returned to work and women more often reached disability pension (χ2 = 13.6; df = 3; P < 0.01).
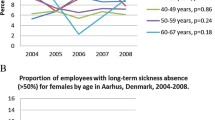
Men and women of age groups <35 years, 35–44 years, 45–54 years and ≥55 years were distinguished. Figure 1 shows the life table survival function of episodes with depressive symptoms in each of these subgroups.

Survival function of the duration of absence due to depression in men and women by age
Women with depressive symptoms had a lower return to work rate than men. After 26 weeks 53.0% were still absent as compared to 48.8% in men. More women (25.5%) than men (22.3%) reached the disability pension date. In Table 2 the results of the Kaplan–Meier estimation are presented by age, company size and sector. The estimation of the mean duration of absence due to depressive symptoms (with a maximum of one year) was 200 (median 179) days in men and 213 (median 201) days in women.
In all age categories, women with depressive symptoms were absent longer than men. Elderly employees had a longer duration of absence and a higher risk of reaching disability. Employees in companies with less than 75 employees were absent for a longer period than employees working in large sized companies. Employees in the educational and public sector had the longest absence duration, followed by employees in commercial services and health care. Men working in the industrial sector had the shortest duration of absence due to depressive symptoms.
Table 3 shows the mean number of absence days corrected for part-time return to work. Men with depressive symptoms had significantly less absence days than women: 154 and 165 absence days, respectively (T = −5.3; df = 9,844; P < 0.01). Because the mean percentage of part-time return to work was almost equal in men and women, this was due to a shorter duration of absence episodes in men. Elderly employees with depressive symptoms had more absence days than younger employees (F(3, 9,862) = 16.5; P < 0.01), because of a longer duration of the absence episodes and lower part-time return to work percentages. The post hoc Tukey test revealed that the difference was significant in employees aged 35 years and more as compared to younger employees.
Among employees working in companies with more than 5,000, we found more part-time return to work than in smaller companies, resulting in a relatively low mean number of corrected absence days (F(3, 9,344) = 14.7; P < 0.01). The post hoc Tukey test revealed that three subsets based on decreasing number of absence days could be distinguished: companies with less that 75 employees, companies with 75–5,000 employees and companies with more than 5,000 employees. The difference in mean number of absence days between the sectors was significant (F(8, 9,880) = 8.2; P < 0.01). According to the post hoc Tukey test, employees in the educational and public sector had the highest number of absence days corrected for part-time return to work. Employees in the transportation and communication sector had a significantly lower number of absence days as compared to the other sectors.
Discussion
Our study showed that depressed women were absent longer from work than men, which confirmed our first hypothesis (H1). The mean duration of absenteeism due to depressive symptoms was 213 (median 201) days in women and 200 (median 179) days in men. This could be due to gender differences in the severity of the depressive symptoms. However, no gender differences were found in the duration of depressive episodes in a population sample (Eaton et al. 1997) and in the severity or symptomatology of depressive disorders in general practice (Hildebrandt et al. 2003).
In studies on absence and depression, reverse gender differences are found. For sickness absence in general, women have more sickness absence days than men (Harrison and Martocchio 1998; Kivimäki et al. 2003; Central Statistical Office of the Netherlands 2006). According to Laitinen-Krispijn and Bijl (2000), depression was a stronger risk factor for absence in men than in women. However, Hensing et al. (1996, 2000) found a higher incidence of absence due to psychiatric disorders in women as compared to men. Hensing et al. (1996, 2000) even found longer absence durations for men with psychiatric disorders as compared to women. They reported about neurosis, and we investigated depressive symptoms, which might explain part of the difference.
Hensing et al. (1996, 2000) reported that the longer duration of absence among men could be explained by gender differences in co-morbidity with alcohol problems and other psychiatric disorders. They also mentioned gender differences in seeking health care, diagnostic procedures and treatment of psychiatric disorders. The social consequences of having a psychiatric disorder might be worse for men than for women, leading to under-reporting among men. Men might postpone the use of health care and get into a poorer mental condition. As a consequence, they need a longer period of recovery and are absent longer from work. Gender differences in the (assessment of) severity of psychiatric problems might also explain the different duration of sick-leave. However, if these mechanisms do play a role in our study, they are more unfavourable to depressed women than to depressed men.
Dewa et al. (2003) reported that depressed women returned to work more often than men, rather than leaving employment. They defined the end of the absence period as returning to work either part-time or fulltime. In our study men returned more often to work than women. We regarded fulltime return to work as the end of an absence period, because we did not have the exact dates of part-time return to work. It is possible that women returned more often to work part-time than men.
Depressed elderly workers are absent longer than young employees with depressive symptoms, confirming our second hypothesis (H2). Sickness absence increases with age, regardless of diagnosis (North et al. 1993; Marmot et al. 1995). Hensing et al. (2000) found higher rates of absence with psychiatric diagnoses in older ages. Like in our study, the increase they found is less linear than in general absence studies. This can be explained by the fact that sickness absence with a psychiatric diagnosis differs from sickness absence due to other diagnoses, since the duration of absence is long in the youngest age groups as well. Age differences in the severity of psychiatric disorder, in help-seeking behavior, recognition and/or treatment may influence the duration of sick-leave due to depression. An alternative factor, which may contribute to the longer duration, is that elderly employees prefer to retire from the labour force. In contrast with Hensing et al. (1996) we found that men in all age groups, especially in the youngest age groups, had fewer days of sick-leave than women in the corresponding age group. Further study is necessary to investigate these gender differences by age.
In accordance with our third hypothesis (H3), the periods of absence due to depressive symptoms were shorter in large-scale companies than in smaller ones. The reintegration percentage is higher in large companies, resulting in a lower number of absence days. Probably, large companies have more opportunities for part-time return to work. Moreover, large companies have structured protocols as to how to deal with long-term absence from work. In the transportation and communications sectors, part-time return to work was most often observed. In our sample, these are mostly large companies in the postal and telecommunications sector, offering more reintegration possibilities. Although blue-collar workers generally have higher sickness absence than white-collar workers, depressed employees in industrial settings had shorter absence durations. A possible explanation might be that employees in the industrial sector are more susceptible to stigmatization of having mental problems, and return to work earlier. Also, in blue-collar workers, depressive symptoms may more often be masked by or diagnosed as somatic diseases.
Employees in the educational and public sectors had longer duration of depressive episodes, resulting in more absence days, confirming our fourth hypothesis (H4). An explanation is that these employees find it harder to report themselves sick because of the difficulty to substitute their work and the personal ties with their clients and pupils (Aronsson et al. 2000). Probably they have more severe depressive symptoms at the moment of sick-leave. Another explanation for their longer absence might be the lesser reintegration opportunities in these sectors. Finally, the mean age of employees in the educational and public sectors was higher than average, and it is known from Dutch national sickness absence surveys that elderly employees are absent longer than younger ones. More research is needed to examine these possible explanations.
Duration of absence due to depression compared to other absenteeism studies
The duration of absence due to depressive symptoms is longer than reported in international research (Hensing et al. 1996, 2000; Sorvaniemi et al. 2003) and the figures according to the Medical Disability Advisor (2006). Differences in definitions and methods may account for this finding. Hensing et al. (1996) reported on episodes of combined depression and anxiety disorder, exceeding 7 days and without maximum duration. In contrast to our study, they did not censor for the end of the observation period. Hensing et al. (2000) investigated sickness absence due to neurosis with a minimum duration of 15 days until the end of the absence. We investigated absence due to depressive symptoms with a minimum duration of 1 day and maximized at 365 calendar days. In our study, 98% of cases had a minimum absence duration of 15 days. The code depressive symptoms was given in the second or third week of absence, when the absent employee consults the occupational physician.
Sorvaniemi et al. (2003) studied sick-leaves with depression according to DSM-III-R in psychiatric outpatients. They used exact beginning and ending dates of sick-leaves, resulting in durations ranging from 2 to 374 days and a mean duration of 142 days. At this point, it should be reminded that depressive symptoms were not strictly assessed according to the DSM criteria, limiting the comparability of results.
Besides, the occupational physician can only give one diagnosis per absence episode. Comorbidity could not be coded. Approximately two-thirds (64%) of respondents with 12-month major depressive disorder meet the criteria for at least one other mental disorder, with anxiety disorders (58%) more common than substance abuse (9%) or impulse control (17%) (Kessler et al. 2003). Comorbidity may substantially prolong the duration of an absence episode. The long duration of absence due to depressive symptoms might be explained by comorbid features. Alternatively, it is possible that depressive symptoms were reactive to somatic disease. In case the symptoms of somatic disease appeared first, the occupational physician encoded the somatic disease and not the reactive depressive symptoms. During sick-leave, the occupational physician evaluates the medical situation and recovery every 6 weeks. Bias can only be expected when the somatic disease was not known in the sick-leave period of the depressed worker. Further investigation of the influence of comorbidity by more detailed research of the medical files is necessary, as Chisholm et al. (2003) reported that the economic consequences of depression (e.g. number of lost work days) were influenced to a greater extent by the presence of medical comorbidity than by symptom severity alone.
Duration of a depressive episode compared to the duration of absence
The median duration of absence due to depression in our study exceeds the estimations of duration of depressive episodes in the general Dutch population (Spijker et al. 2002). In a population survey, Kessler et al. (2003) found a mean duration of a depressive episode of 16 weeks using the composite international diagnostic interview (CIDI). This is about half of our estimated duration of absence. Population studies may underestimate the duration of a depressive disorder, because adults with severe forms of depression are less likely to participate in such studies (Centers for Disease Control and Prevention 2004). Studies on the duration of a depressive episode using the additional life chart interview showed a mean duration of 26 weeks in men and 27 weeks in women (Eaton et al. 1997). This corresponds to the mean absence durations we found: 28.6 weeks in depressed men and 30.4 weeks in depressed women. Blazer et al. (1994) found an overall mean duration of 22.6 weeks by means of a diagnostic interview. For the purpose of their analysis, however, 3% of the participants who had had very long episodes were excluded.
When chronic cases are considered, our estimates were comparable to the study of Spijker et al. (2002) in the general population. They found a chronic course (duration 12 months or more) in 24% of cases. Our survival analysis also indicated a chronic course in 24% of cases. It is important to investigate which employees are at risk for a chronic course.
The duration of a depressive episode in The Netherlands is comparable to other countries, whereas the duration of absenteeism is longer. It could be hypothesized that Dutch employees return to work when they are completely recovered, while in other countries employees start working (part-time) during recovery. We think that differences in social legislation and benefits contribute to these differences. In most other European countries compensation schemes apply to work-related diseases (“risque professional”). In The Netherlands, however, the social insurance system does not take into account the cause of the disease (“risque social”). Moreover, social benefits could have contributed to the relatively long absence duration. Dutch employers are obliged to pay the employee on sick-leave at least 70% of his/her salary. In almost all cases the full salary is paid during the first year of sick-leave, which does not motivate employees to return to their work.
Limitations of the study
Our population is not a random sample from the total Dutch working population, because employers voluntarily engage our occupational health department. Therefore, results are not representative of the whole Dutch working population. However, the considerable sample size and the use of registered, rather than self-rated information on sickness absence, are strong points of this study.
A depressive episode was diagnosed in employees who visited the occupational physician. Persons with lower grade depressive moods might not have reported complaints, and stayed at work. If absent, they might have returned to work before they consulted the occupational physician. Alternatively, they might have called off a visit to the occupational physician, because they intended to resume their work soon. Therefore, more severe cases of depression were included in our sample. The duration of absence due to depressive symptoms is related to the severity of depression (Dewa et al. 2003).
We investigated the interaction between depression and work sectors, but could not examine the influence of work content and working conditions. Rugulies et al. (2006) reported work environment to influence the risk of developing severe depressive symptoms. Work factors also influence the probability of returning to work once absent (North et al. 1996; Väänänen et al. 2003; Nielsen et al. 2004).
Clinical implications
-
Because of the risk of chronicity, it is important that occupational physicians recognize depressive symptoms in an early stage of the absence episode
-
It is recommended to develop and apply tools for recognizing employees at risk for chronic depression
-
Special attention should be given to employees in educational and public services, commercial services and health care as they are at risk for longer absence duration in case of depressive symptoms.
Study limitations
-
Diagnosis of depressive symptoms in absent employees may be biased towards absences with a longer duration. Mildly depressed employees, who did not report ill or returned to work before consulting the occupational physician, were not included
-
Depressive symptoms were not strictly assessed according to DSM criteria, limiting the comparability to other studies
-
Our absence registration system does not account for comorbidity.
Notes
For absences starting from January 1 2004 this period is expanded to two years, but in our study the 1-year limit is applied to all absences, except in the life table results.
References
Aronsson G, Gustafsson K, Dallner M (2000) Sick but yet at work. An empirical study of sickness presenteeism. J Epidemiol Community Health 54:502–509
Blazer DG, Kessler RC, McGonagle KA, Swartz MS (1994) The prevalence and distribution of major depression in a national community sample: the National Comorbidity Survey. Am J Psychiatry 151:979–986
Blossfeld HP, Rohwer G (2002) Techniques of event history modeling. New approaches to causal analysis. Lawrence Erlbaum Associates Inc., Mahwah, pp 39–42
Centers for Disease Control and Prevention (2004) Self-reported frequent mental distress among adults––United States. JAMA 292:2458–2459
Central Statistical Office of the Netherlands (2006) Arbeid en sociale zekerheid [Labour and social security]. Heerlen/Voorburg, The Netherlands. Available at: http://www.statline.cbs.nl. Accessed 14 Feb 2006
Chisholm D, Diehr P, Knapp M, Patrick D, Treglia M, Simon G (2003) Depression status, medical comorbidity and resource costs: evidence from an international study of major depression in primary care (LIDO). Br J Psychiatry 183:121–131
Coryell W, Akiskal HS, Leon AC, Winokur G, Maser JD, Mueller TI, Keller MB (1994) The time course of nonchronic major depressive disorder. Uniformity across episodes and samples. Arch Gen Psychiatry 51:405–410
Dewa CS, Hoch JS, Lin E, Paterson M, Goering P (2003) Pattern of antidepressant use and duration of depression-related absence from work. Br J Psychiatry 183:507–513
Eaton WW, Anthony JC, Gallo J, Cai G, Tien A, Romanoski A, Lyketsos C, Chen L-S (1997) Natural history of diagnostic interview schedule/DSM-IV major depression. The Baltimore epidemiologic catchment area follow-up. Arch Gen Psychiatry 54:993–999
Furukawa TA, Kiturama T, Takahashi K (2005) Time to recovery of an inception cohort with hitherto untreated unipolar major depressive episodes. Br J Psychiatry 177:331–335
Harrison DA, Martocchio JJ (1998) Time for absenteeism: a 20-year review of origins, offshoots, and outcomes. J Manage 24:305–330
Hensing G, Alexanderson K, Allebeck P, Bjurulf P (1996) Sick-leave due to psychiatric disorder––higher incidence among women and longer duration for men. Br J Psychiatry 169:740–746
Hensing G, Brage S, Nygård JF, Sandanger I, Tellnes G (2000) Sickness absence with psychiatric disorders––an increased risk for marginalisation among men? Soc Psychiatry Psychiatr Epidemiol 35:335–340
Hildebrandt MG, Stage KB, Kragh-Soerensen P (2003) Gender and depression: a study of severity and symptomatology of depressive disorders (ICD-10) in general practice. Acta Psychiatr Scand 107:197–202
Kaplan EL, Meier P (1958) Nonparametric estimation from incomplete observations. J Am Stat Assoc 53:457–481
Keller MB, Shapiro RW, Lavori PW, Wolfe N (1982) Recovery in major depression. Analysis with life tables and regression models. Arch Gen Psychiatry 39:905–910
Kendler KS, Walters EE, Kessler RC (1997) The prediction of length of major depressive episodes: results from an epidemiological sample of female twins. Psychol Med 27:107–117
Kessler RC, Frank RG (1997) The impact of psychiatric disorders on work loss days. Psychol Med 27:861–873
Kessler RC, Barber C, Birnbaum HG, Frank RG, Greenberg PE, Rose RM, Simon GE, Wang P (1999) Depression in the workplace: effects on short-term disability. Health Aff 18:163–171
Kessler RC, Berglund P, Demler O, Jin R, Koretz D Merikangas KR, Rush AJ, Walters EE, Wang PS (2003) The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 289:3095–3105
Kivimäki M, Head J, Ferrie JE, Shipley MJ, Vahtera J, Marmot MG (2003) Sickness absence as a global measure of health: evidence from mortality in the Whitehall II prospective cohort study. Br Med J 327:364–368
Kouzis AC, Eaton WW (1994) Emotional disability days: prevalence and predictors. Am J Public Health 84:1304–1307
Laitinen-Krispijn S, Bijl RV (2000) Mental disorders and employee sickness absence: the NEMESIS study. Soc Psychiatry Psychiatr Epidemiol 35:71–77
Marmot M, Feeney A, Shipley M, North F, Syme SL (1995) Sickness absence as a measure of health status and functioning: from the UK Whitehall II study. J Epidemiol Community Health 49:124–130
Medical Disability Advisor Internet, 5th Edition. Major Depression. Reed Group. http://www.mdainternet.com [accessed April 03 2006]
Mueller TI, Keller MB, Leon AC, Solomon DA, Shea MT, Coryell W, Endicott J (1996) Recovery after 5 years of unremitting major depressive disorder. Arch Gen Psychiatry 53:794–799
Nielsen ML, Rugulies R, Christensen KB, Smith-hansen L, Bjorner JB, Kristensen TS (2004) Impact of the psychosocial work environment on registered absence from work: a two-year longitudinal study using the IPAW cohort. Work Stress 18:323–335
Nieuwenhuijsen K, Verbeek JH, de Boer AG, Blonk RW, van Dijk FJ (2006) Predicting the duration of sickness absence for patients with common mental disorders in occupational health care. Scand J Work Environ Health 32:67–74
North FM, Syme SL, Feeney A, Shipley M, Marmot M (1993) Explaining socioeconomic differences in sickness absence: the Whitehall II study. Br Med J 306:61–66
North FM, Syme SL, Feeney A, Shipley M, Marmot M (1996) Psychosocial work environment and sickness absence among British civil servants: the Whitehall II study. Am J Public Health 86:332–340
Raddjoe R, van der Hoek W (2005) Verzuimduur bij depressie [Duration of absence due to depression]. Tijdschrift voor Bedrijfs-en Verzekeringsgeneeskunde 13:272
Rugulies R, Bültmann U, Aust B, Burr H (2006) Psychosocial work environment and incidence of severe depressive symptoms: prospective findings from a 5-year follow-up of the Danish work environment cohort study. Am J Epidemiol 163:877–887
Skodol AE, Schwartz S, Dohrenwend BP, Levav I, Shrout PE (1994) Minor depression in a cohort of young adults in Israel. Arch Gen Psychiatry 51:542–551
Solomon DA, Keller MB, Leon AC, Mueller TI, Shea MT, Warshaw M, Maser JD, Coryell W, Endicott J (1997) Recovery from major depression. A 10-year prospective follow-up across multiple episodes. Arch Gen Psychiatry 54:1001–1006
Sorvaniemi M, Helenius H, Salokangas RKR (2003) Sickleave certificates granted to psychiatric outpatients with major depression. Depress Anxiety 17:220–223
Spijker J, de Graaf R, Bijl RV, Beekman AT, Ormel J, Nolen WA (2002) Duration of major depressive episodes in the general population: results from The Netherlands Mental Health Survey and Incidence Study (NEMESIS). Br J Psychiatry 181:208–213
Väänänen A, Toppinen-Tanner S, Kalimo R, Mutanen P, Vahtera J, Peiro JM (2003) Job characteristics, physical and psychological symptoms, and social support as antecedents of sickness absence among men and women in the private industrial sector. Soc Sci Med 57:807–824
World Health Organization (2002) Mental and neurological disorders. Indian J Med Sci 56:25–29
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Koopmans, P.C., Roelen, C.A.M. & Groothoff, J.W. Sickness absence due to depressive symptoms. Int Arch Occup Environ Health 81, 711–719 (2008). https://doi.org/10.1007/s00420-007-0243-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-007-0243-7