
Abstract
Background
Chronic central serous chorioretinopathy is a serious therapeutic problem as it may lead to significant visual impairment. The aim of this retrospective study is to evaluate functional and morphological effects, as well as factors influencing visual outcome in patients treated by subthreshold micropulse laser.
Methods
Fifty-one eyes with chronic central serous chorioretinopathy lasting longer than 4 months (18 months on average) underwent up to two sessions of subtreshold micropulse laser treatment. Change in best corrected visual acuity, central retinal thickness, central retinal volume, average central retinal thickness and maximum subretinal fluid height were measured. Relation between the effects of the treatment and the initial retinal morphological and functional parameters was then analyzed.
Results
The total resorption of subretinal fluid was achieved in 36 cases (70.6%). There was, however, only a minor improvement in best corrected visual acuity of approximately one line on the Snellen chart. No correlation was observed between the effects of the treatment and the duration of the symptoms, retinal morphology and initial visual acuity. Younger patients responded better to the therapy.
Conclusion
Subthreshold micropulse laser treatment in chronic serous chorioretinopathy provides good morphological results, however significant improvement of visual acuity is not to be expected.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Central serous chorioretinopathy (CSCR) is a fairly common, well-described clinical entity [1,2,3]. For the most part, it presents in an acute form, in which symptoms recede spontaneously after a few months. This form of CSCR has a good prognosis and does not impair visual acuity. In its chronic form, however, CSCR poses a real threat to quality of vision, the majority of patients ending up with some form of visual defect, usually a moderate decrease in best corrected visual acuity (BCVA), metamorphopsia or scotoma. A significant decrease in BCVA is noted in a minority of cases, however, for most patients the symptoms of the disease are very alarming and often prevent them from participating in their everyday professional activity [4,5,6,7]. It should also be stressed that CSCR normally affects young and active people, for whom even a moderate visual disturbance is significant. Moreover, this clinical entity is largely associated with type A personality, hence the reason why, for some patients, CSCR symptoms are simply unbearable [8, 9].
Treatments for CSCR have been sought for many years, with laser photocoagulation of the leakage point representing a practical solution in selected cases of longer duration [10, 11]. In such cases the leakage point was required to be located at a safe distance from the center of the fovea. Despite observance of this rule, however, some patients have complained of visual scotomas after undergoing such therapy. In addition to this method, practitioners have looked to numerous types of oral medication in search of a resolution for CSCR symptoms (antibiotics, non-steroidal anti-inflammatory drugs, acetazolamide, rifampin, low doses of aspirin, etc.). However, any results they have obtained have not been confirmed in randomized trials [12,13,14,15,16]. Just recently, mineralocorticoid pathway inhibitors have been tested in CSCR treatment with promising results [17,18,19]. Photodynamic therapy (PDT) is an important form of treatment of chronic CSCR, which is, nevertheless, costly and unavailable in some regions [20,21,22,23,24]. Use of a 689-nm wavelength laser with verteporfin in the PDT procedure was also attempted alone in the treatment of CSCR. The study comparing results of PDT treatment and sole 689 nm laser treatment of CSCR showed that both procedures were equally effective; however, it included cases of relatively short duration of CSCR (17-19 weeks) [25]. The efficacy of anti-VEGF treatment in chronic CSCR is disputable [26,27,28,29], with recent data failing to confirm its superiority over PDT or other therapies [30, 31].
In light of these clinical experiences, subthreshold micropulse laser treatment (SMPLT) represents an opportunity for a cheap and effective form of therapy.
The abovementioned type of therapy has been used for treatment of CSCR for the last few years with promising results. In the micropulse mode the energy of the laser is delivered to the tissues in the train of very short repetitive impulses. Effective time of the laser impact is described as duty cycle and for retinal diseases usually set at as low as 5%. The idea of application of subthreshold micropulse laser is stimulation of the RPE to production of antiangiogenic factors without damage to the sensory retina. In consequence, intraretinal or subretinal fluid is easier to be absorbed. Photothermal effect is limited to the RPE only, and due to subthreshold and micropulse modes, is minimal [32,33,34]. Properly performed SMPLT leaves the sensor retina without any trace, neither visible nor detectable by fundus autofluorescence (FAF) or fluorescein angiography (FA).
This study attempted to analyze results of SMPLT treatment in chronic CSCR, as well as determine factors that could influence functional and morphological outcome. The objective was to find a possible correlation between the effects of SMPLT and the following parameters: age of patient, duration of symptoms, retinal morphology before treatment (retinal thickness and amount of subretinal fluid), and initial visual acuity.
Material and methods
All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration. The study included 51 patients with chronic CSCR, who had been treated with SMPLT at our outpatient ophthalmological clinic during the last 2 years. CSCR was considered chronic when symptoms persisted for longer than 4 months. The 51 patients treated were made up of 17 women (33.3%) and 34 men (66.7%), the age of the patients ranging from 32 to 80 years, with an average of 53.8 years +/- 11.2. The duration of CSCR extended from 4 to 72 months, giving an average of 18.4 months +/- 17.6. Distribution of patients according to age and duration of CSCR is presented in Table 1.
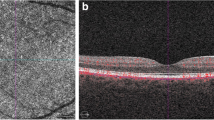
None of the patients had previously undergone any invasive treatment due to CSCR, such as laser photocoagulation or photodynamic therapy; however, some of the patients were earlier treated by oral or topical non-steroidal drugs or troxerutin without therapeutic success. Prior to the treatment, all cases were subject to observation in other clinics. Diagnostic criterion of CSCR was the presence of subretinal fluid (SRF), sometimes accompanied by pigment epithelial detachment (PED), in the absence of choroidal neovascularization (CNV). CSCR was diagnosed by spectral optical coherence tomography (SOCT, Cirrus 4000, Zeiss, Germany 2012), fluorescein angiography, and fundus autofluorescence (FF-450, Zeiss, Germany 2010). The presence of SRF was determined by SOCT and FA. FAF was used to reveal changes in retinal pigment epithelium (RPE) typical for chronic CSCR, so-called gravitational tracks, places of lipofuscin accumulation in the RPE cells and RPE loss. Choroidal neovascularization was excluded by FA. Angio-OCT and indocyanine green angiography was not at our disposal during the study. Patients suspected of having CNV were excluded. All patients underwent a full ophthalmological examination, which included a review of their medical history and measurements of BCVA on a Snellen chart. For statistical analysis results were converted into log MAR scale. SOCT was used for determining the following parameters: central retinal thickness (CRT), central retinal volume (cube volume, CV), average central retinal thickness (CRTA) and maximum SRF height. In all cases SRF was found to be present under the foveola, however, in some eyes its maximum height was not located exactly at the center of the macula. Therefore, it deemed advisable to find additional parameter to measure the maximum change in retinal morphology after SMPLT.
BCVA and SOCT parameters were measured both prior to treatment and 2 months after each SMPLT. In cases where satisfactory results were not observed 2 months after the first SMPLT (residual subretinal fluid was still present), another SMPLT session was scheduled in 1 month’s time (hence a 3-month interval between the SMPLT sessions). BCVA and SOCT measurements were then taken once again 2 months after the second SMPLT. Analysis of the material was made after a maximum of two laser sessions. During the SMPLT procedure, the whole SRF area was covered with confluent foci of micropulse yellow laser (577nm) (Supra Scan 577, Quantel Medical, France 2014), based on the SOCT retinal maps. The focus diameter was set at 160 μm, power at a fixed level of 250mW, time of exposure at 0.2 s, and duty cycle at 5%.
Statistical analysis
The primary measure of effectiveness of the SMPLT was percentage of patients with total resolution of subretinal fluid after maximum of two sessions of subthreshold micropulse laser. Secondary measures were decrease in the value of retinal parameters: CRT, CRTA, CV and SRF height and improvement of BCVA. Statistical analysis was conducted by Wilcoxon test.
For correlation between success of SMPLT (total resolution of SRF) and baseline patient characteristics, the values of different morphological and functional parameters before treatment were compared between the group of patients with total resolution of SRF and the group of eyes where SRF was still present after SMPLT. Difference in mean values of CRT, CRTA, CV, SRF height, BCVA, age of patient, and duration of CSCR between those two groups was measured. Analysis of statistical significance of the differences between two means was performed using U Mann-Whitney test.
Additionally, the influence of duration of CSCR on the potential morphological and functional improvement after SMPLT was also analyzed.
For that purpose, OCT measurements and BCVA were evaluated in the group of patients who responded well to SMPLT (total resolution of SRF) in the relation to the duration of CSCR. This group was divided into two subgroups: one with duration of CSCR up to 12 months (18 eyes) and the second with duration of CSCR above 12 months (33 eyes). One year seemed long enough to demonstrate eventual influence of the longstanding presence of subretinal fluid on retinal architecture. The mean results of the SOCT measurements (CRT, CRTA, CV, maximum fluid height) and BCVA after SMPLT were compared between those two subgroups. Statistical significance of the difference of two means was evaluated by U Mann-Whitney test and t-Student test.
Statistical analysis was performed using Statistica 10.0 (StatSoft Inc., 2011), and the following primary parameters of descriptive statistics were selected: arithmetic mean (M), median (Me), standard deviation (SD), first and third quartiles (Q1 and Q3) and the minimum (Min) and maximum (Max) values. The assumed distribution of variables compatibility with normal distribution were tested by the Shapiro-Wilk. The statistical hypotheses were verified using the t-Student test, Mann-Whitney U test and Wilcoxon test. The results were quantified statistically significant in cases where the calculated probability satisfied the inequality test, p <0.05.
Results
The results of SPMLT are presented in Table 2. The change in all presented SOCT parameters and BCVA was statistically significant. The average values show a reduction of retinal edema as well as the volume of SRF. The improvement of visual acuity is not, however, spectacular at equivalent to approximately one line on the Snellen chart. The complete resorption of SRF was achieved in 36 cases (70.6%). In remaining 18 cases SRF was still present after two sessions of SMPLT. Among patients with complete resorption of SRF only five required second sessions of SMPLT (13,9%).
Table 3 presents the difference in baseline morphological and functional parameters between the group of patients with total resolution of SRF after SMPLT and the group of patients with SRF still present after the treatment. This chart presents also difference in age and duration of symptoms between these groups (Table 3).
A statistically significant correlation was found between the age of patients and their morphological response to SMPLT. Patients with complete resolution of subretinal fluid were significantly younger than patients with persistent SRF after SMPLT (accordingly M=51.5 years SD=11.0 and M=59.3 years SD=9.9). A correlation between the duration of CSCR and retinal thickness was also observed - a general cognition being that sensory retina gets thinner as CSCR progresses. This change in retinal morphology can be measured in patients with absolute resolution of SRF after SMPLT (Table 4).
As can be observed from the data, all retinal parameters are lower in patients who had CSCR for a longer period of time however there is no statistically significant difference in BCVA.
Discussion
SMPLT has been used intensively for the treatment of retinal edema of various origins during the last few years [35,36,37]. Clinical entities treated by SMPLT include diabetic macular edema (DME), CSCR, retinal edema secondary to retinal vein occlusion (RVO), or even exudative macular degeneration. The morphological results are usually promising. However, in a certain percentage of cases SMPLT does not have the expected effect, especially regarding improvement of BCVA. In the treatment of DME authors recommend the use of SMPLT for smaller edemas of less than 400 μm [38,39,40,41]. So far, recommendations for the use of SMPLT in CSCR are not unequivocal and it is not clear which patients could benefit the most from this treatment. Hence, the interest on our part in evaluating factors that could influence the outcome of this treatment. To our knowledge it is the first study to evaluate these factors in the same fashion, as it is usually done with other clinical entities, such as AMD or DME. Other authors have reported SMPLT efficacy in CSCR measured as reduction of retinal thickness and improvement of BCVA. Luttrull achieved the resolution of SRF after SMPLT in 11 cases of relatively short duration of CCSR (up to 7 months) [42]. Abd Elhamid reported a significant improvement in CRT and contrast sensitivity in 15 eyes with CSCR lasting 4.6 months on average [43]. Scholz et al. had morphological improvement rate of 74% in 38 cases of chronic CSCR including patients unresponsive to PDT [44]. Others reported short-term efficacy of SMPLT in reducing the CRT in relatively small groups of patients (10 to 15 eyes) with CSCR [45,46,47]. Özmert and Scholz compared SMPLT treatment to PDT in CSCR therapy showing better morphological results in laser treatment. [48, 49]
Table 5 presents number of eyes and type of treated cases in recent studies.
Nevertheless, it should be stressed that in some studies researchers treat both chronic and acute cases, which could have resolved spontaneously without any treatment. It is clear that establishing adequate criteria for chronicity of CSCR is important when evaluating the results of SMPLT. This study dealt with genuine chronic cases, the average duration of CSCR amounting to 18 months. Moreover, in comparison to other studies, this study is based on a reasonably large sample size, which allows the relevant statistical analysis to be carried out.
The study included patients with CSCR in the form of SRF, sometimes accompanied by PED. Cases of chronic pure PED without SRF, which could have been treated as chronic CSCR, were also initially included as part of the sample; however, poor response to SMPLT treatment in such cases (20% success rate) led to the conclusion that they were in fact a form of RPE degeneration, and not an active form of CSCR, hence their exclusion from this study.
Our study’s results show high efficacy of SMPLT in providing resolution of SRF in chronic CSCR. Complete resolution of subretinal fluid is in our opinion sensible criterion of morphological success of the procedure. Cases that show a just a reduction in SRF height after SMPLT, are in our opinion not resolved cases. The persistence of even small amounts of SRF in the long term might lead to progressive retinal thinning and the loss of photoreceptors. Such conclusions have been confirmed by the analysis of the group of patients who experienced the complete resolution of SRF after SMPLT. In cases of longer duration of CSCR, that is more than 12 months, a decrease in retinal morphological parameters, such as CRT or CV was observed.
Generally, SMPLT improved retinal morphology however the improvement noted in BCVA is small, what remains in consent with results of other studies. [44,45,46] Significant improvement in BCVA was noted in the studies that included acute cases, which probably improved more than the chronic ones [42, 43]. It might be true that cases of CSCR of duration longer than 4 months generally do not improve well functionally. Theoretically, a longer duration of symptoms should correlate with lower BCVA before and after treatment. Nevertheless, this was not found to be the case for the whole group in our study. Hence, major visual loss may occur in the first months following the onset of symptoms and may not progress in a linear way during the following months. The logical conclusion that can be drawn from this, is that SMPLT treatment should be considered sooner than 4 months after onset of CSCR, especially in cases that do not show tendency for spontaneous resolution.
The study was not successful in explaining why some eyes do not react to SMPLT, with no correlation between response to treatment and duration of CSCR, initial BCVA or initial CRT being found. It is reasonable to assume that the answer lies in the retinal and choroidal morphology; however, this is yet to be determined. CSCR is not a disease, which follows the same logic as other retinal vascular clinical entities, such as retinal vein occlusion or DME. The loss of vision associated with the disease is not linear and the response to the treatment does not resemble that of DME or RVO. Nevertheless, at present SMPLT should be taken into consideration as an option for treatment of acute CSCR that do not show tendency for SRF reduction.
It remains uncertain whether SMPLT can be used in the prevention of the recurrence of CSCR. However, in our study during the 9 months of follow up no recurrence of SRF was observed.
SMPLT has to be compared with other pulse type of lasers of shorter pulse duration such as selective retina therapy (SRT). The goal of this kind of treatment is to selectively damage the RPE and stimulate proliferation and migration of the adjacent RPE cells into the damage site. In consequence, due to rejuvenation of the diseased sites, metabolism of the RPE improves, enabling elimination of the intraretinal or subretinal fluid [50]. Elsner et al. treated 27 patients with active CSCR with pulsed double-Q-switched Nd-YLF prototype laser (lambda=527 nm, t=1.7 micros) achieving resolution of SRF in 85.2% of cases [51]. Framme et al. treated relatively small group of acute (10 eyes) and chronic (16 eyes) CSCR cases with the same type of laser, but shorter pulse duration [52]. Complete SRF resolution was noted in all acute cases after 3 months. In chronic cases one laser session brought complete SRF resolution in 19% of treated eyes; however, retreatment with higher pulse energy resulted in success in 83.3% of the remaining chronic CSCR cases. BCVA improvement in chronic cases was minor (from 71.6 to 72.8 letters ETDRS. Park tested the efficacy of SRT with automated real-time feedback-controlled dosimetry in 50 eyes with chronic CSCR [53]. SRF resolved completely in 74% at 3 months with mean BCVA improvement from 0.44 to 0.37 logMAR. Results of SRT in chronic CSCR are similar to those achieved by SMPLT in both retinal morphology and BCVA change. Application of SRT results in similar percentage of patients with complete SRF resolution and, same as in SMPLT, only minor BCVA improvement. With the advent of commercially available SRT lasers, this kind of therapy might be also considered an option in the treatment of chronic CSCR; however, its cost has to be taken into consideration.
Conclusions
Subthreshold micropulse is an effective form of therapy in improving retinal morphology in chronic CSCR. Functional results of SMPLT in longstanding CSCR are poor. In order to achieve good visual results, SMPLT may be considered in acute cases showing no tendency for spontaneous improvement. The prolonged presence of SRF leads to retinal thinning and loss of visual acuity.
The explicit factors that determine the effects of SMPLT in CSCR are yet to be identified, and, in all probability, are awaiting discovery within the field of ocular morphology.
References
Spaide RF, Campeas L, Haas A, Yannuzzi LA, Fisher YL, Guyer DR et al (1996) Central serous chorioretinopathy in younger and older adults. Ophthalmology 103:2070–2079
Gemenetzi M, De Salvo G, Lotery AJ (2010) Central serous chorioretinopathy: an update on pathogenesis and treatment. Eye 24:1743–1756
Daruich A, Matet A, Dirani A, Bousquet E, Zho M, Farman N et al (2015) Central serous chorioretinopathy: Recent findings and new physiopathology hypothesis. Progress in Retinal and Eye Research 48:82–118
Pare JR, Guo Y, Schechter-Perkins EM (2014) The evaluation of acute vision loss: central serous chorioretinopathy. Am J Emerg Med 32:396.e3–396.e4
Liew G, Quin G, Gillies M, Fraser-Bell S (2013) Central serous chorioretinopathy: a review of epidemiology and pathophysiology. Clin Exp Ophthalmol 41:201–214
Salehi M, Wenick AS, Law HA, Evans JR, Gehlbach P (2015) Interventions for central serous chorioretinopathy: a network meta-analysis. Cochrane Database Syst Rev 22:CD011841
Wong KH, Lau KP, Chhablani J, Tao Y, Li Q, Wong IY (2016) Central serous chorioretinopathy: what we have learnt so far. Acta Ophthalmol 94:321–325
Liu B, Deng T, Zhang J (2016) Risk factors for central serous chorioretinopathy: A Systematic Review and Meta-Analysis. Retina 36:9–19
Lahousen T, Painold A, Luxenberger W, Schienle A, Kapfhammer HP, Ille R (2016) Psychological factors associated with acute and chronic central serous chorioretinopathy. Nord J Psychiatry 70:24–30
Khosla PK, Rana SS, Tewari HK, Azad RU, Talwar D (1997) Evaluation of visual function following argon laser photocoagulation in central serous retinopathy. Ophthalmic Surg Lasers 28:693–697
Gass JDM (1987) Stereoscopic Atlas of Macular Diseases: Diagnosis and Treatment, 3rd edn. Mosby, St. Louis, pp 46–59
Shulman S, Goldenberg D, Schwartz R, Habot-Wilner Z, Barak A, Ehrlich N et al (2016) Oral Rifampin treatment for longstanding chronic central serous chorioretinopathy. Graefes Arch Clin Exp Ophthalmol 254:15–22
Pouw AE, Olmos de Koo LC (2015) Oral rifampin for central serous retinopathy: a strategic approach in three patients. Ophthalmic Surg Lasers Imaging Retina 46:98–102
Caccavale A, Romanazzi F, Imparato M, Negri A, Morano A, Ferentini F (2010) Low-dose aspirin as treatment for central serous chorioretinopathy. Clin Ophthalmol 4:899–903
Caccavale A, Imparato M, Romanazzi F, Negri A, Porta A, Ferentini F (2009) A new strategy of treatment with low-dosage acetyl salicylic acid in patients affected by central serous chorioretinopathy. Med Hypotheses 73:435–437
Chong CF, Yang D, Pham TQ, Liu H (2012) A novel treatment of central serous chorioretinopathy with topical anti-inflammatory therapy. BMJ Case Rep. 2012 pii: bcr2012006970
Salz DA, Pitcher JD III, Hsu J, Regillo CD, Fineman MS, Elliott KS, Vander JF, Fischer DH, Spirn MJ (2015) Oral eplerenone for treatment of chronic central serous chorioretinopathy: a case series. Ophthalmic Surg Lasers Imaging Retina 46:439–444
Daruich A, Matet A, Dirani A, Gallice M, Nicholson L, Sivaprasad S, Behar-Cohen F (2016) Oral Mineralocorticoid-Receptor Antagonists: Real-Life Experience in Clinical Subtypes of Nonresolving Central Serous Chorioretinopathy With Chronic Epitheliopathy. Transl Vis Sci Technol 4(5):2
Kapoor KG, Wagner AL (2016) Mineralocorticoid Antagonists in the Treatment of Central Serous Chorioretinopathy: A Comparative Analysis. Ophthalmic Res 56:17–22
Kretz FT, Beger I, Koch F, Nowomiejska K, Auffarth GU, Koss MJ (2015) Randomized Clinical Trial to Compare Micropulse Photocoagulation Versus Half-dose Verteporfin Photodynamic Therapy in the Treatment of Central Serous Chorioretinopathy. Ophthalmic Surg Lasers Imaging Retina 46:837–843
Breukink MB, Mohr JK, Ossewaarde-van Norel A, den Hollander AI, Keunen JE, Hoyng CB et al (2016) Half-dose photodynamic therapy followed by diode micropulse laser therapy as treatment for chronic central serous chorioretinopathy: evaluation of a prospective treatment protocol. Acta Ophthalmol 94:187–197
Alkin Z, Perente I, Ozkaya A, Alp D, Agca A, Aygit ED, Korkmaz S, Yazici AT, Demirok A (2014) Comparison of efficacy between low-fluence and half-dose verteporfin photodynamic therapy for chronic central serous chorioretinopathy. Clin Ophthalmol 8:685–690
Lim JI, Glassman AR, Aiello LP, Chakravarthy U, Flaxel CJ, Spaide RF (2014) Macula Society CSC Collaborative Study Group. Research and Education Committee and Website Committee. Collaborative retrospective macula society study of photodynamic therapy for chronic central serous chorioretinopathy. Ophthalmology 121:1073–1078
Yannuzzi LA, Slakter JS, Gross NE, Spaide RF, Costa D, Huang SJ et al (2003) Indocyanine green angiography-guided photodynamic therapy for treatment of chronic central serous chorioretinopathy: a pilot study. Retina 23:288–298
Russo A, Turano R, Morescalchi F, Gambicorti E, Cancarini A, Duse S, Costagliola C, Semeraro F (2017) Comparison of half-dose photodynamic therapy and 689 nm laser treatment in eyes with chronic central serous chorioretinopathy. Graefes Arch Clin Exp Ophthalmol 255:1141–1148
Lim JW, Ryu SJ, Shin MC (2010) The effect of intravitreal bevacizumab in patients with acute central serous chorioretinopathy. Korean J Ophthalmol 24:155–158
Ünlü C, Erdogan G, Aydogan T, Sezgin Akcay BI, Kardes E, Kiray GA, Bozkurt TK (2016) Intravitreal Bevacizumab for Treatment of Central Serous Chorioretinopathy. J Ophthalmic Vis Res 11:61–65
Altun A, Kurna SA, Olcaysu OO, Sengor T, Aki SF, Atakan TG (2014) Success of ranibizumab in central serous chorioretinopathy resistant to bevacizumab. J Ocul Pharmacol Ther 30:842–846
Park SU, Lee SJ, Kim M (2014) Intravitreal anti-vascular endothelial growth factor versus observation in acute central serous chorioretinopathy: one-year results. Korean J Ophthalmol 28:306–313
Koss MJ, Beger I, Koch FH (2012) Subthreshold diode laser micropulse photocoagulation versus intravitreal injections of bevacizumab in the treatment of central serous chorioretinopathy. Eye 26:307–314
Bae SH, Heo J, Kim C, Kim TW, Shin JY, Lee JY et al (2014) Low-fluence photodynamic therapy versus ranibizumab for chronic central serous chorioretinopathy: one-year results of a randomized trial. Ophthalmology 121:558–565
Barnstable CJ, Tombran-Tink J (2004) Neuroprotective and antiangiogenic actions of PEDF in the eye: molecular targets and therapeutic potential. Prog Ret Eye Res 23:561–577
Glaser BM, Campochiaro PA, Davis JL et al (1987) Retinal pigment epithelial cells release inhibitors of neovascularization. Ophthalmology 94:780–784
Pollack JS, Kim JE, Pulido JS, Burke JM (1998) Tissue effects of subclinical diode laser treatment of the retina. Arch Ophthalmol 116:1633–1639
Luttrull JK, Sramek C, Palanker D, Spink CJ, Musch DC (2012) Long-term safety,high-resolution imaging, and tissue temperature modeling of subvisible diode micropulse photocoagulation for retinovascular macular edema. Retina 32:375–386
Brader HS, Young LH (2016) Subthreshold Diode Micropulse Laser: A Review. Semin Ophthalmol 31:30–39
Luttrull JK, Chang DB, Margolis BW, Dorin G, Luttrull DK (2015) Laser resensitization of medically unresponsive neovascular age-related macular degeneration : Efficacy and implications. Retina 35:1184–1194
Luttrull JK, Musch DC, Mainster MA (2005) Subthreshold diode micropulse photocoagulation for the treatment of clinically significant diabetic macular oedema. Br J Ophthalmol 89:74–80
Vujosevic S, Martini F, Convento E, Longhin E, Kotsafti O, Parrozzani R et al (2013) Subthreshold laser therapy for diabetic macular edema: metabolic and safety issues. Curr Med Chem 20:3267–3271
Vujosevic S, Martini F, Longhin E, Convento E, Cavarzeran F, Midena E (2015) Subthreshold micropulse yellow laser versus subthreshold micropulse infrared laser in center-involving diabetic macular edema: Morphologic and Functional Safety. Retina 35:1594–1603
Vujosevic S, Bottega E, Casciano M, Pilotto E, Convento E, Midena E (2010) Microperimetry and fundus autofluorescence in diabetic macular edema:subthreshold micropulse diode laser versus modified early treatment diabetic retinopathy study laser photocoagulation. Retina 30:908–916
Luttrull JK (2015) Low-intensity/high-density subthreshold diode micropulse laser for central serous chorioretinopathy. Retina 36:1658–1663
Abd Elhamid AH (2015) Subthreshold micropulse yellow laser treatment for nonresolving central serous chorioretinopathy. Clin Ophthalmol 9:2277–2283
Scholz P, Ersoy L, Boon CJ, Fauser S (2015) Subthreshold Micropulse Laser (577 nm) Treatment in Chronic Central Serous Chorioretinopathy. Ophthalmologica 234:189–194
Yadav NK, Jayadev C, Mohan A, Vijayan P, Battu R, Dabir S et al (2015) Subthreshold micropulse yellow laser (577 nm) in chronic central serous chorioretinopathy: safety profile and treatment outcome. Eye 29:258–264
Kim JY, Park HS, Kim SY (2015) Short-term efficacy of subthreshold micropulse yellow laser (577-nm) photocoagulation for chronic central serous chorioretinopathy. Graefes Arch Clin Exp Ophthalmol 253:2129–2135
Malik KJ, Sampat KM, Mansouri A, Steiner JN, Glaser BM (2015) Low-intensity/high-density subthreshold microPulse diode laser for chronic central serous chorioretinopathy. Retina 35:532–536
Özmert E, Demirel S, Yanık Ö, Batıoğlu F (2016) Low-Fluence Photodynamic Therapy versus Subthreshold Micropulse Yellow Wavelength Laser in the Treatment of Chronic Central Serous Chorioretinopathy. J Ophthalmol 2016:3513794
Scholz P, Altay L, Fauser S (2016) Comparison of subthreshold micropulse laser (577 nm) treatment and half-dose photodynamic therapy in patients with chronic central serous chorioretinopathy. Eye 30:1371–1377
Brinkmann R, Schüle G, Neumann J, Framme C, Pörksen E, Elsner H, Theisen-Kunde D, Roider J, Birngruber R (2006) Selective retina therapy: methods, technique, and online dosimetry. Ophthalmologe. 103:839–849
Elsner H, Pörksen E, Klatt C, Bunse A, Theisen-Kunde D, Brinkmann R, Birngruber R, Laqua H, Roider J (2006) Selective retina therapy in patients with central serous chorioretinopathy. Graefes Arch Clin Exp Ophthalmol. 244:1638–1645
Framme C, Walter A, Berger L, Prahs P, Alt C, Theisen-Kunde D, Kowal J, Brinkmann R (2015) Selective Retina Therapy in Acute and Chronic-Recurrent Central Serous Chorioretinopathy. Ophthalmologica 234:177–188
Park YG, Kang S, Kim M, Yoo N, Roh YJ (2017) Selective retina therapy with automatic real-time feedback-controlled dosimetry for chronic central serous chorioretinopathy in Korean patients. Graefes Arch Clin Exp Ophthalmol 255:1375–1383
Funding
No funding was received for this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study (retrospective study) formal consent is not required.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Gawęcki, M., Jaszczuk-Maciejewska, A., Jurska-Jaśko, A. et al. Functional and morphological outcome in patients with chronic central serous chorioretinopathy treated by subthreshold micropulse laser. Graefes Arch Clin Exp Ophthalmol 255, 2299–2306 (2017). https://doi.org/10.1007/s00417-017-3783-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-017-3783-x