
Abstract
Background
Post-cataract endophthalmitis has increased after introduction of clear cornea incisions (CCI). Laboratory models suggested that these incisions might not be competent at certain changes in intraocular pressure (IOP). Considering that side-port incisions (SPI) might behave similarly, the purpose of the present study was to determine the most stable side-port incision configuration.
Methods
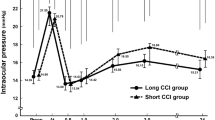
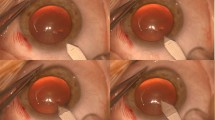
Using four cadaveric human eyes, four different side-port incisions (SPI) were created in each cornea: 1.5 mm and 2.5 mm squared tunnel, 1.5 mm and 2.5 mm stab tunnel. Fluorescein was placed on the eye, and the IOP varied from 10 to 80 mmHg. IOP at which each SPI started leaking was recorded. In the second part of the study, India ink was applied to the corneal surface at normal IOP, and then rinsed with balanced salt solution (BSS). The ink influx was recorded by planimetry. IOP was elevated to 80 mmHg, ink was reapplied, and IOP was dropped to 0 mmHg. Ink influx was measured again. Histological examination was used to visualize ink inflow into each incision.
Results
There was no statistically significant difference in the IOP levels at which the different incisions leaked (p = 0.52). A significant increase in the length of India ink ingress in all incision types was measured after IOP variation (p < 0.05). The 2.5 mm squared incision showed the least increase in ink inflow in this test.
Conclusion
All incision types of SPIs tested exhibited similar resistance to leakage after IOP variation. Good resistance to wound leakage may not predict adequate resistance to the inflow of bacterial-sized particles into the wound.




Similar content being viewed by others

References
Taban M, Behrens A, Newcomb RL, Nobe MY, Saedi G, Sweet PM, McDonnell PJ (2005) Acute endophthalmitis following cataract surgery: systematic review of the literature. Arch Ophthalmol 123:613–620
Fine IH (1994) Clear corneal incisions. Int Ophthalmol Clin 34:59–72
Olson RJ, Mamalis N, Werner L, Apple DJ (2003) Cataract treatment in the beginning of the 21st century. Am J Ophthalmol 136:146–154
Maxwell DP Jr, Diamond JG, May DR (1994) Surgical wound defects associated with endophthalmitis. Ophthalmic Surg 25:157–161
West ES, Behrens A, McDonnell PJ, Tielsch JM, Schein OD (2005) The incidence of endophthalmitis after cataract surgery among the U.S Medicare population increased between 1994 and 2001. Ophthalmology 112:1388–1394
Shingleton BJ, Wadhwani RA, O’Donoghue MW, Baylus S, Hoey H (2001) Evaluation of intraocular pressure in the immediate period after phacoemulsification. J Cataract Refract Surg 27:524–527
Herretes S, Stark WJ, Pirouzmanesh A, Reyes JM, McDonnell PJ, Behrens A (2005) Inflow of ocular surface fluid into the anterior chamber after phacoemulsification through sutureless corneal cataract wounds. Am J Ophthalmol 140:737–740
Coleman DJ, Trokel S (1969) Direct-recorded intraocular pressure variations in a human subject. Arch Ophthalmol 82:637–640
McDonnell PJ, Taban M, Sarayba M, Rao B, Zhang J, Schiffman R, Chen Z (2005) Dynamic morphology of clear corneal cataract incisions. Ophthalmology 110:2342–2348
Taban M, Rao B, Reznik J, Zhang J, Chen Z, McDonnel PJ (2004) Dynamic morphology of sutureless cataract wounds—effect of incision angle and location. Surv Ophthalmol Suppl 2:S62–S72
Calladine D, Packard R (2007) Clear corneal incision architecture in the immediate postoperative period evaluated using optical coherence tomography. J Cataract Refract Surg 33:1429–1435
Chee SP (2005) Clear corneal incision leakage after phacoemulsification — detection using povidone iodine 5%. Int Ophthalmol 26:175–179
Chee SP, Ti SE, Lim L, Chan AS, Jap A (2010) Anterior segment optical coherence tomography evaluation of the integrity of clear corneal incisions: a comparison between 2.2 mm and 2.65 mm main incisions. Am J Ophthalmol 149:768–776
Kau HC, Cc T, Kao SC, Hsu WM, Liu JH (2002) Corneal ulcer of the side port after phacoemulsification induce by Acinetobacter baumanii. J Cataract Refract Surg 28:895–897
Khedi EE, Watson SL, Fracis IC, Chong R, Bank A, Coroneo MT, Dart JK (2005) Spectrum of clear corneal incision cataract wound infection. J Cataract Refract Surg 1702–1706
Diggle PJ, Heagerty P, Liang KY, Zeger SL (2002) Generalized linear models for longitudinal data. In: Analysis of longitudinal data. Oxford University Press, Oxford; pp 138–140
Chawdhary S, Anand A (2006) Early post-phacoemulsification hypotony as risk factor for intraocular contamination: in vivo model. J Cataract Refract Surg 32:609–613
Stratas BA (2005) Clear corneal paracentesis: a case of chronic wound leakage in a patient having bimanual phacoemulsification. J Cataract Refract Surg 31:1075
Sarayba MA, Taban M, Ignacio TS, Behrens A, McDonnell PJ (2004) Inflow of ocular surface fluid through clear corneal cataract incisions: a laboratory model. Am J Ophthalmol 138:206–210
May W, Castro-Combs J, Camacho W, Wittmann P, Behrens A (2008) Analysis of clear corneal incision integrity in an ex vivo model. J Cataract Refract Surg 34:1013–1018
Taban M, Sarayba MA, Ignacio TS, Behrens A, McDonnell PJ (2005) Ingress of India ink into the anterior chamber through sutureless clear corneal cataract wounds. Arch Ophthalmol 123:643–648
Nichamin LD, Chang DF, Johnson SH, Mamalis N, Masket S, Packard RB, Rosenthal KJ, American Society of Cataract and Refractive Surgery Cataract Clinical Committee (2006) ASCRS white paper: what is the association between clear corneal cataract incisions and postoperative endophthalmitis? J Cataract Refract Surg 32:1556–1559
Ernest PH, Lavery KT, Kiessling LA (1994) Relative strength of scleral and corneal incisions constructed in cadaver eyes. J Cataract Refract Surg 20:626–629
Acknowledgment
This work supported in part by an unrestricted grant from Research to Prevent Blindness Inc. (New York, NY, USA) to The Wilmer Eye Institute, and by NIH.
Data analyses were supported by Wilmer Biostatistics Core Grant EY01765 NIH/NEI.
Financial disclosure
Authors have no financial interest in any of the devices or drugs used in the study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Authors have full control of all primary data, and we agree to allow Graefe’s Archive for Clinical and Experimental Ophthalmology to review our data upon request.
Rights and permissions
About this article
Cite this article
Kashiwabuchi, F.K., Khan, Y.A., Rodrigues, M.W. et al. Seidel and India ink tests assessment of different clear cornea side-port incision configurations. Graefes Arch Clin Exp Ophthalmol 251, 1961–1965 (2013). https://doi.org/10.1007/s00417-013-2380-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-013-2380-x