
Abstract
Background
To evaluate the ability of scanning laser polarimetry with variable corneal compensation (GDx-VCC) in separating healthy from glaucomatous patients with early visual field (VF) loss.
Methods
Sixty-two healthy and 48 glaucomatous age-matched patients with early glaucoma [mean deviation (MD): −1.74dB ±1.69] underwent complete ophthalmological evaluation, automated achromatic perimetry (AAP) and retinal nerve fiber layer (RNFL) measurement with GDx-VCC. One randomly selected eye from each subject was considered. Glaucomatous VF defects had either Glaucoma Hemifield Test (GHT) outside normal limits or pattern standard deviation (PSD) outside 95% confidence limits. Mean (±SD) MD, PSD and GDx-VCC parameters in the two groups were compared by t-test. For each GDx-VCC parameter, area under receiver operating characteristics (AUROC) curve and sensitivity at predetermined specificity ≥80% and ≥95% were calculated. Moreover, the parameter with largest AUROC was evaluated by likelihood ratios (LRs).
Results
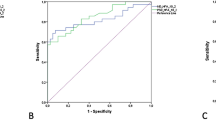
Mean values for MD, PSD and ten of 14 GDx-VCC parameters were significantly different between the two groups (P<0.001). The three parameters with largest AUROCs were the nerve fiber indicator (NFI) (0.870), superior average (0.817) and normalized superior area (0.816) (P=0.08 for differences between AUROCs). NFI displayed sensitivity values of 80.2% and 60.4% for specificity ≥80% and ≥95%, respectively. At NFI cutoff value of 30, positive LR was 34.9 (95% CI: 4.9–247.6) and negative LR was 0.45 (95% CI: 0.32–0.61). Interval LRs showed large effect on post-test probability for NFI values ≤18 or ≥31.
Conclusions
In our sample of eyes with early VF loss, GDx-VCC showed moderate-to-good discriminating ability. Among the best performing parameters, NFI had the largest AUROC, but several glaucomatous eyes (21, 43.8%) had NFI <30. This suggests that algorithm for NFI calculation requires some refinement when eyes with early VF loss are evaluated.

Similar content being viewed by others


References
Bagga H, Greenfield DS, Feuer WJ, Knighton RW (2003) Scanning laser polarimetry with variable corneal compensation and optical coherence tomography in normal and glaucomatous eyes. Am J Ophthalmol 135:521–529
Bowd C, Zangwill LM, Berry CC, Blumenthal EZ, Vasile C, Sanchez-Galeana C et al (2001) Detecting early glaucoma by assessment of retinal nerve fiber layer thickness and visual function. Invest Ophthalmol Vis Sci 42:1993–2003
Bowd C, Zangwill LM, Weinreb RN (2003) Association between scanning laser laser polarimetry measurements using variable corneal polarization compensation and visual field sensitivity in glaucomatous eyes. Arch Ophthalmol 121:961–966
Choplin NT, Zhou Q, Knighton RW (2003) Effect of individualized compensation for anterior segment birefringence on retinal nerve fiber layer assessment as determined by scanning laser polarimetry. Ophthalmology 110:719–725
Gallagher EJ (2003) Evidence-based emergency medicine/editorial: the problem with sensitivity and specificity. Ann Emerg Med 42:298–303
Greenfield DS, Knighton RW, Huang XR (2000) Effect of corneal polarization axis on assessment of retinal nerve fiber layer thickness by scanning laser polarimetry. Am J Ophthalmol 129:715–722
Greenfield DS, Knighton RW, Feuer WJ, Schiffmann JC, Zangwill LM, Weinreb RN (2002) Correction for corneal polarization axis improves the discriminating power of scanning laser polarimetry. Am J Ophthalmol 134:27–33
Hanley JA, McNeil BJ (1983) A method for comparing the areas under receiver operating characteristics curves derived from the same cases. Radiology 148:839–843
Hodapp E, Parrish RK II, Anderson DR (1993) Clinical decisions in glaucoma. Mosby, St. Louis, pp 52–61
Jaeschke R, Guyatt GH, Sackett DL (1994) Evidence-Based Medicine Working Group. User’s guides to the medical literature, III: how to use an article about a diagnostic test, B: what are the results and will they help me in caring for my patients? JAMA 271:703–707
Kass MA, Heuer DK, Higginbotham EJ, Johnson CA, Keltner JL, Miller JP et al (2002) The ocular hypertension treatment study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol 120:701–713
Knighton RW, Huang XR (2002) Linear birefringence of the central human cornea. Invest Ophthalmol Vis Sci 43:82–86
Medeiros FA, Susanna R Jr (2003) Comparison of algorithms for detection of localised nerve fiber layer defects using scanning laser polarimetry. Br J Ophthalmol 87:413–419
Medeiros FA, Zangwill LM, Bowd C, Bernd AS, Weinreb RN (2003) Fourier analysis of scanning laser polarimetry measurements with variable corneal compensation in glaucoma. Invest Ophthalmol Vis Sci 44:2606–2612
Medeiros FA, Zangwill LM, Bowd C, Weinreb RN (2004) Comparison of the GDx VCC scanning laser polarimeter, HRT II confocal scanning laser ophthalmoscope, and Stratus OCT optical coherence tomography for the detection of glaucoma. Arch Ophthalmol 122:827–837
Pederson JE, Anderson DR (1980) The mode of progressive optic disc cupping in ocular hypertension and glaucoma. Arch Ophthalmol 98:490–495
Quigley HA, Addicks EM, Green RW (1982) Optic nerve damage in human glaucoma. III. Quantitative correlation of nerve fiber loss and visual defect in glaucoma, ischemic neuropathy, papilledema, and toxic neuropathy. Arch Ophthalmol 100:15–146
Reus NJ, Colen TP, Lemij HG (2003) Visualization of localized retinal nerve fiber layer defects with the GDx with individualized and with fixed compensation of anterior segment birefringence. Ophthalmology 110:1512–1516
Reus NJ, Lemij HG (2004) Diagnostic accuracy of the GDx VCC for glaucoma. Ophthalmology 111:1860–1865
Reus NJ, Lemij HG (2004) The relationship between standard automated perimetry and GDx VCC measurements. Invest Ophthalmol Vis Sci 45:840–845
Reus NJ, Lemij HG (2004) Scanning laser polarimetry of the retinal nerve fiber layer in perimetrically unaffected eyes of glaucoma patients. Ophthalmology 111:2199–2203
Schlottmann PG, De Cilla S, Greenfield DS, Caprioli J, Garway-Heath DF (2004) Relationship between visual field sensitivity and retinal nerve fiber layer thickness as measured by scanning laser polarimetry. Invest Ophthalmol Vis Sci 45:1823–1829
Simel DL, Samsa GP, Matchar DB (1991) Likelihood ratios with confidence: sample size estimation for diagnostic test studies. J Clin Epidemiol 44:763–770
Sommer A, Katz J, Quigley HA, Miller NR, Robin AL, Richter RC et al (1991) Clinically detectable nerve fiber layer atrophy precedes the onset of glaucomatous field loss. Arch Ophthalmol 109:77–83
Tannenbaum D, Hoffmann D, Lemij HG, Garway-Heath DF, Greenfield DS, Caprioli J (2004) Variable corneal compensation improves the discrimination between normal and glaucomatous eyes with the scanning laser polarimeter. Ophthalmology 111:259–264
Weinreb RN, Dreher AW, Coleman A, Quigley H, Shaw B, Reiter K (1990) Histopathologic validation of Fourier-ellipsometry measurements of retinal nerve fiber layer thickness. Arch Ophthalmol 108:557–560
Weinreb RN, Bowd C, Zangwill LM (2002) Glaucoma detection using scanning laser polarimetry with variable corneal polarization compensation. Arch Ophthalmol 120:218–224
Weinreb RN, Bowd C, Greenfield DS, Zangwill LM (2002) Measurement of the magnitude and axis of corneal polarization with scanning laser polarimetry. Arch Ophthalmol 120:901–906
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Da Pozzo, S., Fuser, M., Vattovani, O. et al. GDx-VCC performance in discriminating normal from glaucomatous eyes with early visual field loss. Graefe's Arch Clin Exp Ophthalmo 244, 689–695 (2006). https://doi.org/10.1007/s00417-005-0144-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-005-0144-y