
Abstract
Background
During retinal photocoagulation for diabetic maculopathy, there is a potential risk of foveal burns, and laser scars may later enlarge to be sight-threatening when involving retinal areas previously used during fixation. Since the retinal area used during binocular steady fixation has been found to vary considerably in the normal test person and central fixation may be even further compromised in patients with diabetic maculopathy, the sight-threatening side effects could possibly be reduced by taking into account the fixation area individually. However, no study has described and quantified the retinal area of fixation binocularly in patients with clinically significant macular oedema (CSME).
Methods
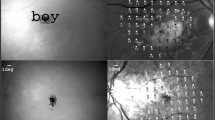
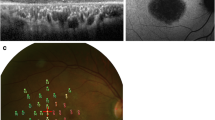
Sixteen diabetic patients with CSME in one or both eyes were examined. Each examination included visual acuity testing (ETDRS charts), a standard eye examination, central retinal thickness assessment by optical coherent tomography, fluorescein angiography and binocular quantification of fixational eye movements using an infrared recording technique.
Results
A negative correlation was found between visual acuity and mean microsaccadic amplitude (R=0.48, p=0.009). The maximal retinal extension of the fixation area ranged between 1.0° and 3.0°, and in two eyes with CSME, this area was estimated to exceed 800 μm on the retinal plane. No correlation was found between retinal thickness and visual acuity, retinal area of fixation, maximal extension of the fixation area or mean microsaccadic amplitude.
Conclusion
Large interindividual differences in quantitative measures of binocular fixational eye movements were found. The mean amplitude of fixational eye movements was not correlated to central retinal thickness, and fixation area could only partly be predicted by visual acuity. Two eyes with CSME had an estimated maximal extension of the fixation area exceeding the central 800 μm on the retinal plane; thus, the possible benefit of individualising central photocoagulation according to precise measures of fixation area needs to be investigated on a larger population.






Similar content being viewed by others

References
Acosta F, Lashkari K, Reynaud X, Jalkh AE, Van de Velde, Chedid (1991) Characterisation of functional change in macular holes and cysts. Ophthalmology 98:1820–1823
Amos AF, McCarty DJ, Zimmet P (1997) The rising global burden of diabetes and its complications; estimates and projections to year 2010. Diabet Med 14(suppl 5):1–85
Cornsweet TN (1956) Determination of the stimuli for involuntary drifts and saccadic eye movements. J Opt Soc Am 46:987–993
Culham LE, Fitzke FW, Timberlake GT, Marshall J (1993) Assessment of fixation stability in normal subject and patients using a scanning laser ophthalmoscope. Clin Vis Sci 8:551–561
Curcio CA, Sloan KR, Packer O, Hendrickson AE, Kalina RE (1987) Distribution of cones in human and monkey retina: individual variability and radial asymmetry. Science 236:579–581
Curcio CA, Sloan KR, Kalina RE, Hendrickson AE (1990) Human photorecepter topography. J Comp Neurol 292:497–523
Early Treatment Diabetic Reinopathy Study Research Group (1985) Photocoagulation for diabetic macular edema Early treatment diabetic reinopathy study research group report number 1. Arch Ophthalmol 103:1796–1806
Farber DB, Flannery JG, Lolley RN and Bok (1985) Distribution patterns of photoreceptors, proteins and cyclic nucleotides in the human retina. Investig Ophthalmol Vis Sci 26:1558–1568
Green A, Andersen PK, Svendsen AJ, Mortensen K (1992) Increasing incidence of early onset type 1 (insulin dependent diabetes mellitus) diabetes mellitus: a study of Danish male birth cohorts. Diabetologia 35(2):178–182
Green A, Sjølie AK, Eshøj O (1996) Trends in the epidemiology of IDDM during 1970–2020 in Fyn County, Denmark. Diabetes Care 19(8):801–806
Hamstra SJ, Sinha T, Hallett PE (2001) The joint contribution of saccades and ocular drifts to repeated ocular fixations. Vis Res 41:1709–1721
Jampel RA, Shi DX (2000) Retinal micromovements, the visual line, and Donders’ law. Am J Ophthalmol 129:224–234
Kinyoun J, Barton F, Fischer M, Hubbard L, Aiello L, Ferris F (1989) Detection of diabetic macular edema. Ophthalmoscopy versus photography-Early Treatment Diabetic Retinopathy Study Report 5. The ETDRS Research Group. Ophthalmology 96(6):746–750
Kosik W, Fikre J, Sekuler R (1986) Visual fixation stability in older adults. Investig Ophthalmol Vis Sci 27:1720–1725
Kowler E, Steinman RN (1979) Miniature saccades: eye movements that do not count. Vis Res 19:105–108
Kowler E, Steinman RN (1980) Small saccades serve no useful purpose. Vis Res 20:271–272
Krauskopf J, Cornsweet TN, Riggs LA (1960) Analysis of eye movements during monocular and binocular fixation. J Opt Soc Am 50:572–578
Leopold DA, Longothesis NK (1998) Microsaccades differentially modulate neural activity in the striate and extrastriate cortex. Exp Brain Res 123(3):341–345
Löwenstam-Adrian M, Agardh E (2000) Photocoagulation of diabetic macular oedema; complications and visual outcome. Acta Ophthalmol Scand 78(6):667–671
Martinez-Conde S, Macknik SL, Hubel DH (2000) Microsaccadic eye movements and firing of single cells in the striate cortex of macaque monkeys. Nat Neurosci 3(3):251–258
Martinez-Conde, Macknik S, Hubel DH (2002) The function of bursts of spikes during visual fixation in the awake primate lateral geniculate nucleus and primary visual cortex. Proc Natl Acad Sci USA 99(21):13920–13925
Martinez-Conde, Macknik S, Hubel DH (2004) The role of fixational eye movements in perception. Nat Rev Neurosci 5(3):229–240
Massin P, Vicaut E, Haouchine B, Erginay A, Paques M, Gaudric A (2001) Reproducibility of retinal mapping using optical coherent tomography. Arch Ophthalmol 119(8):1135–1142
Møller F, Sjølie AK, Bek T (1996) Quantitative assessment of fixational eye movements by scanning laser ophthalmoscopy. Acta Ophthalmol Scand 74(6):578–583
Møller F, Bek T (1998) The relation between visual acuity and the size of fixational eye movements in patients with diabetic and non-diabetic macular disease. Acta Ophthalmol Scand 76:38–42
Møller F, Bek T (2000) Lack of correlation between visual acuity and fixation stability after photocoagulation for diabetic maculopathy. Graefe Arch Clin Exp Ophthalmol 238(7):566–570
Møller F, Laursen ML, Thygesen J, Sjølie AK (2002) Binocular quantification and characterization of microsaccades. Graefe Arch Clin Exp Ophthalmol 204:765–770
Møller F, Bek T (2003) The relation between visual acuity, fixation stability, and the size and location of foveal hard exudates after photocoagulation for diabetic maculopathy. A 1 year follow-up study. Graefe Arch Clin Exp Ophthalmol 241(6):458–462
Møller F, Laursen ML, Sjølie AK (2004) Fixation topography in normal test persons. Graefe Arch Clin Exp Ophthalmol (in press)
Olk RJ (1986) Modified grid argon (blue-green) laser photocoagulation for diffuse macular edema. Ophthalmology 93(7):938–950
Tasman W, Jaeger E (1993) Duane’s clinical ophthalmology, vol. 1, chapter 33, revised edition. J.B. Lippincott Company, Philadelphia, USA
Weih LM, VanNewkirk MR, McCarthy CA, Taylor HR (2000) Age-specific causes of bilateral visual impairment. Arch Ophthalmol 118(2):264–269
Winterson BJ, Collewijn H (1976) Microsaccades during finely guided visiomotor tasks. Vis Res 16:1387–1390
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Møller, F., Laursen, M.L. & Sjølie, A.K. Binocular fixation topography in patients with diabetic macular oedema. Graefe's Arch Clin Exp Ophthalmol 243, 903–910 (2005). https://doi.org/10.1007/s00417-004-1120-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-004-1120-7