
Abstract
Purpose
Because of the rarity of peripunctal tumours and their clinical classification as conjunctival or eyelid tumours, they have gained little attention in the literature. We conducted a retrospective study to illustrate the different clinical and histopathological spectrum of peripunctal tumours seen at two oculoplastics clinics.
Methods
In a retrospective interventional clinicopathologic case series study, all the charts of patients with peripunctal tumours presented at an ophthalmic oncology clinic in Jerusalem, Israel and an oculoplastics clinic in Boston, USA were reviewed. The tumours were classified as epithelial and non-epithelial tumours. The symptoms caused by these tumours, their pattern of growth and their management were evaluated.
Results
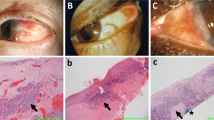
Fourteen peripunctal tumours were identified. Eleven out of 175 (6.3%) peripunctal disorders and out of approximately 4, 000 (0.27%) surgical oculoplastics patients were seen at Massachusetts Eye & Ear Infirmary, Boston. Three were seen at Hadassah University Hospital, Jerusalem. Seven histopathological types of peripunctal tumours of epithelial, subepithelial or melanocytic origin causing punctal occlusion or displacement were identified. The tumours included compound and junctional naevi, non-pigmented compound naevus, epithelial, subepithelial inclusion cysts, verrucous and squamous papilloma, pyogenic granuloma and oncocytoma. All the tumours were benign. They involved the peripunctal or canalicular epithelium, the adjacent skin, the glandular epithelium or the subepithelium. They presented as a peripunctal mass or were accidentally disclosed but none of them resulted in epiphora.
Conclusions
Peripunctal tumours are rare. They exhibit different clinical types of growth and may be difficult to diagnose based on their clinical appearance alone. The location of peripunctal tumours potentially allows their extension from the conjunctival sac into the canaliculus and vice versa. Therefore, it is best to ascertain free margins when the tumour is excised.







Similar content being viewed by others


References
Annual report (1931) Giza Memorial Ophthalmic Laboratory, Annual Report 5. Schindler Press, Cairo, Egypt, p 35
Kersten RC, Ewing-Chow D, Kulwin DR, Gallon M (1997) Accuracy of clinical diagnosis of cutaneous eyelid lesions. Ophthalmology 104:479–484
Khan JA, Grove AS Jr, Joseph MP, Goodman M (1989) Sebaceous carcinoma, diuretic use, lacrimal system spread, and surgical margins. Ophthalmic Plast Reconstruct Surg 5:227–234
Morel X, Meyer A, Le-Rouic JF (2002) Naevus naevocellulaire achrome palpebral prenant l’aspect d’un carcinome basocellulaire. J Fr Ophtalmol 25:657–660
Moro F (1947) Nevo papillomatoso della papilla lacrimale. Ann Ottal Clin Ocul 73:608–622
Pe’er J, Neufeld M, Ilsar M (1993) Peripunctal eyelid oncocytoma. Am J Ophthalmol 116:385–387
Scott KR, Jakobiec FA, Font RL (1989) Peripunctal melanocytic nevi. Distinctive clinical findings and differential diagnosis. Ophthalmology 96:994–998
Stefanyszyn MA, Hidayat AA, Pe’er J, Flanagan JC (1994) Lacrimal sac tumours. Ophthalmic Plast Reconst Surg 10:169–184
Vrabec J (1966) Naevus puncti lacrimalis. Sb Lek 68:274–278
Author information
Authors and Affiliations
Additional information
Presented in part at the 104th American Academy of Ophthalmology Meeting, Dallas, Texas, October 2000
Rights and permissions
About this article
Cite this article
Rumelt, S., Pe’er, J. & Rubin, P.A.D. The clinicopathological spectrum of benign peripunctal tumours. Graefe's Arch Clin Exp Ophthalmol 243, 113–119 (2005). https://doi.org/10.1007/s00417-004-0907-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-004-0907-x