
Abstract
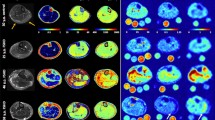
To assess the presence and persistence of muscular edema and increased myoplasmic sodium (Na+) concentration in Duchenne muscular dystrophy (DMD). We examined eight DMD patients (mean age 9.5 ± 5.4 years) and eight volunteers (mean age 9.5 ± 3.2 years) with 3-tesla proton (1H) and 23Na density-adapted 3D-radial MR sequences. Seven DMD patients were re-examined about 7 months later without change of therapy. The eighth DMD patient was re-examined after 5 and 11 months under medication with eplerenone. We quantified muscle edema on STIR images with background noise as reference and fatty degeneration on T1-weighted images using subcutaneous fat as reference. Na+ was quantified by a muscular tissue Na+ concentration (TSC) sequence employing a reference containing 51.3 mM Na+ with 5 % agarose. With an inversion-recovery (IR) sequence, we determined mainly the myoplasmic Na+. The normalized muscular 23Na IR signal intensity was higher in DMD than in volunteers (n = 8, 0.75 ± 0.07 vs. 0.50 ± 0.05, p < 0.001) and persisted at second measurement (n = 7, 1st 0.75 ± 0.07, 2nd 0.73 ± 0.06, p = 0.50). When compared to volunteers (25.6 ± 2.0 mmol/l), TSC was markedly increased in DMD (38.0 ± 5.9 mmol/l, p < 0.001) and remained constant (n = 7, 1st 37.9 ± 6.4 mmol/l, 2nd 37.0 ± 4.0 mmol/l, p = 0.49). Muscular edema (15.6 ± 3.5 vs. 6.9 ± 0.7, p < 0.001) and fat content (0.48 ± 0.08 vs. 0.38 ± 0.01, p = 0.003) were elevated in DMD when compared to volunteers. This could also be confirmed during follow-up (n = 7, p = 0.91, p = 0.12). Eplerenone slightly improved muscle strength and reduced muscular sodium and edema. The permanent muscular Na+ overload in all DMD patients is likely osmotically relevant and responsible for the persisting, mainly intracellular muscle edema that may contribute to the progressive muscle degeneration.

Similar content being viewed by others


References
Bushby K, Finkel R, Birnkrant DJ et al (2010) Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial management. Lancet Neurol 9:77–93
Marden FA, Connolly AM, Siegel MJ, Rubin DA (2005) Compositional analysis of muscle in boys with Duchenne muscular dystrophy using MR imaging. Skeletal Radiol 34:140–148
Weber MA, Nagel AM, Jurkat-Rott K, Lehmann-Horn F (2011) Sodium (23Na) MRI detects elevated muscular sodium concentration in Duchenne muscular dystrophy. Neurology 77:2017–2024
Hirn C, Shapovalov G, Petermann O, Roulet E, Ruegg UT (2008) Nav1.4 deregulation in dystrophic skeletal muscle leads to Na+ overload and enhanced cell death. J Gen Physiol 132:199–208
Bodensteiner JB, Engel AG (1978) Intracellular calcium accumulation in Duchenne dystrophy and other myopathies: a study of 567,000 muscle fibers in 114 biopsies. Neurology 28:439–446
Nagel AM, Laun FB, Weber MA, Matthies C, Semmler W, Schad LR (2009) Sodium MRI using a density-adapted 3D radial acquisition technique. Magn Reson Med 62:1565–1573
Nagel AM, Amarteifio E, Lehmann-Horn F et al (2011) 3 tesla sodium inversion recovery magnetic resonance imaging allows for improved visualization of intracellular sodium content changes in muscular channelopathies. Invest Radiol 46:759–766
Dyck PJ, Boes CJ, Mulder D, Millikan C, Windebank AJ, Espinosa R (2005) History of standard scoring, notation, and summation of neuromuscular signs. A current survey and recommendation. J Peripher Nerv Syst 10:158–173
Weber MA, Nielles-Vallespin S, Essig M, Jurkat-Rott K, Kauczor HU, Lehmann-Horn F (2006) Muscle Na+ channelopathies: MRI detects intracellular 23Na accumulation during episodic weakness. Neurology 67:1151–1158
Stobbe R, Beaulieu C (2005) In vivo sodium magnetic resonance imaging of the human brain using soft inversion recovery fluid attenuation. Magn Reson Med 54:1305–1310
Olsen DB, Gideon P, Jeppesen TD, Vissing J (2006) Leg muscle involvement in facioscapulohumeral muscular dystrophy assessed by MRI. J Neurol 253:1437–1441
Jurkat-Rott K, Weber MA, Fauler M et al (2009) K+-dependent paradoxical membrane depolarization and Na+ overload, major and reversible contributors to weakness by ion channel leaks. Proc Natl Acad Sci USA 106:4036–4041
Jurkat-Rott K, Holzherr B, Fauler M, Lehmann-Horn F (2010) Sodium channelopathies of skeletal muscle result from gain or loss of function. Pflugers Arch 460:239–248
Lansman JB, Franco-Obregón A (2006) Mechanosensitive ion channels in skeletal muscle: a link in the membrane pathology of muscular dystrophy. Clin Exp Pharmacol Physiol 33:649–656
Kirschner J, Schessl J, Schara U et al (2010) Treatment of Duchenne muscular dystrophy with cyclosporin A: a randomised, double-blind, placebo-controlled multicentre trial. Lancet Neurol 9:1053–1059
Manzur AY, Kuntzer T, Pike M, Swan A (2008) Glucocorticoid corticosteroids for Duchenne muscular dystrophy. Cochrane Database Syst Rev 1:CD003725
Salinas RA, Alvarez G, Daly F, Ferreira J (2010) Corticosteroids for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev 17:CD001942
Yamamoto T, Ohara A, Nishikawa M, Yamamoto G, Saeki Y (2011) Dexamethasone-induced up-regulation of two-pore domain K(+) channel genes, TASK-1 and TWIK-2, in cultured human periodontal ligament fibroblasts. In Vitro Cell Dev Biol Anim 47:273–279
Ouwerkerk R, Bleich KB, Gillen JS, Pomper MG, Bottomley PA (2003) Tissue sodium concentration in human brain tumors as measured with 23Na MR imaging. Radiology 227:529–537
Chang G, Wang L, Schweitzer ME, Regatte RR (2010) 3D 23Na MRI of human skeletal muscle at 7 tesla: initial experience. Eur Radiol 20:2039–2046
Borthakur A, Hancu I, Boada FE, Shen GX, Shapiro EM, Reddy R (1999) In vivo triple quantum filtered twisted projection sodium MRI of human articular cartilage. J Magn Reson 141:286–290
Acknowledgments
This study was supported by a research grant from the Deutsche Gesellschaft für Muskelkranke e.V. F. Lehmann-Horn is endowed Senior Research Professor of the non-profit Hertie-Foundation. We appreciate the molecular genetics of patient #8 performed by K. Hinderhofer, MD, Institute of Human Genetics, University Hospital, Heidelberg/Germany (Director C.R. Bartram, MD). We also thank A. Behnecke, MD, Institute of Human Genetics, University Hospital, Heidelberg/Germany, H.-M. Meinck, MD, Department of Neurology, University Hospital, Heidelberg/Germany, and M. Sanchez-Albisua, MD, Sozialpädiatrisches Zentrum (SPZ) Tübingen/Germany for referring some patients. We are grateful to the patients and their families for their participation.
Conflicts of interest
The authors report no conflicts of interest and no disclosures.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
Weber, MA., Nagel, A.M., Wolf, M.B. et al. Permanent muscular sodium overload and persistent muscle edema in Duchenne muscular dystrophy: a possible contributor of progressive muscle degeneration. J Neurol 259, 2385–2392 (2012). https://doi.org/10.1007/s00415-012-6512-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-012-6512-8