
Abstract
Recent studies have suggested a diagnostic role of the B-lymphocyte attracting chemokine (CXCL13) in the cerebrospinal fluid (CSF) in Lyme neuroborreliosis (LNB). Our aim was to evaluate diagnostic accuracy of CSF CXCL13 in a cohort of 59 consecutive patients referred to hospital for suspected LNB. Thirty-seven patients were classified as definite LNB and used as the reference standard. Seven were classified as probable, and seven as possible LNB. Eight patients did not fulfil case definitions and were used as controls.
At presentation, CSF CXCL13 was elevated in all patients with definite LNB, as compared to a positive CSF B. burgdorferi (Bb) antibody index (AI) in 33 of 37. Pre-treatment sensitivity of elevated CSF CXCL13 and positive CSF Bb AI was 100 % (95 % CI = 91–100) and 78 % (95 % CI = 75–96) respectively (p = 0.053).
Among the eight control patients, CSF CXCL13 was normal in five and only slightly elevated in three, and Bb AI was negative in five. Specificity of CSF CXCL13 and Bb AI was similar 63 % (95 % CI = 31–86) (p = 1.0).
CSF CXCL13 was elevated in 6/7 patients with probable LNB and 3/7 patients with possible LNB. Bb AI was negative in all these 14 patients.
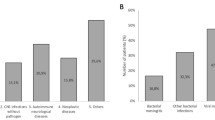
An additional control group consisted of 31 patients with multiple sclerosis (MS), 11 with non-inflammatory neurological diseases, and ten with verified non-Lyme meningitis and high CSF cell count. CSF CXCL13 was slightly elevated in 15 MS patients, and in nine meningitis patients. Mean CSF CXCL13 was higher in definite LNB (3524 ng/g CSF protein) than in MS (27 ng/g) and non-Lyme meningitis (23 ng/g) (p < 0.001).
Four months post-treatment CSF CXCL13 was normalized in 82 % of patients with definite LNB, as compared to a negative Bb AI in 10 % (p < 0.001).
CSF CXCL13 may be a useful supplement in early diagnosis of acute LNB.
Similar content being viewed by others

References
(1997) Case definitions for infectious conditions under public health surveillance. Centers for Disease Control and Prevention. MMWR Recomm Rep 46:1–55
Stanek G, O’Connell S, Cimmino M, Aberer E, Kristoferitsch W, Granstrom M, Guy E, Gray J (1996) European Union Concerted Action on Risk Assessment in Lyme Borreliosis: clinical case definitions for Lyme borreliosis. Wien Klin Wochenschr 108:741–747
(1996) Practice parameter: Diagnosis of patients with nervous system Lyme borreliosis. Report of the Quality Standards Subcommittee of the American Academy of Neurology
Hansen K, Lebech AM (1991) Lyme neuroborreliosis: a new sensitive diagnostic assay for intrathecal synthesis of Borrelia burgdorferi – specific immunoglobulin G, A, and M. Ann Neurol 30:197–205
Tumani H, Nolker G, Reiber H (1995) Relevance of cerebrospinal fluid variables for early diagnosis of neuroborreliosis. Neurology 45:1663–1670
Kaiser R, Rauer S (1998) Analysis of the intrathecal immune response in neuroborreliosis to a sonicate antigen and three recombinant antigens of Borrelia burgdorferi sensu stricto. Eur J Clin Microbiol Infect Dis 17:159–166
Ljostad U, Skarpaas T, Mygland A (2007) Clinical usefulness of intrathecal antibody testing in acute Lyme neuroborreliosis. Eur J Neurol 14:873–876
Hammers-Berggren S, Hansen K, Lebech AM, Karlsson M (1993) Borrelia burgdorferi-specific intrathecal antibody production in neuroborreliosis: a follow-up study. Neurology 43:169–175
Cepok S, Zhou D, Vogel F, Rosche B, Grummel V, Sommer N, Hemmer B (2003) The immune response at onset and during recovery from Borrelia burgdorferi meningoradiculitis. Arch Neurol 60:849–855
Rupprecht TA, Pfister HW, Angele B, Kastenbauer S, Wilske B, Koedel U (2005) The chemokine CXCL13 (BLC): a putative diagnostic marker for neuroborreliosis. Neurology 65:448–450
Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig LM, Lijmer JG, Moher D, Rennie D, de Vet HC (2003) Towards complete and accurate reporting of studies of diagnostic accuracy: the STARD initiative. BMJ 326:41–44
Rupprecht TA, Kirschning CJ, Popp B, Kastenbauer S, Fingerle V, Pfister HW, Koedel U (2007) Borrelia garinii induces CXCL13 production in human monocytes through TLR2. Infect Immun 75(9):4351–4356
Kaiser R (1995) Intrathecal immune response in neuroborreliosis: importance of cross-reactive antibodies. Zentralbl Bakteriol 282:303–314
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article is available at http://dx.doi.org/10.1007/s00415-008-0974-8.
Rights and permissions
About this article
Cite this article
Ljøstad, U., Mygland, Å. CSF B – lymphocyte chemoattractant (CXCL13) in the early diagnosis of acute Lyme neuroborreliosis. J Neurol 255, 732–737 (2008). https://doi.org/10.1007/s00415-008-0785-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-008-0785-y