
Abstract
Purpose
To evaluate how women of child-bearing age perceive the use of remote fetal ECG monitoring technologies. Telemedicine has advanced to the forefront of healthcare delivery, including maternal–fetal medicine. Smart wearable electrocardiogram (ECG) devices can enable pregnant women to monitor their health and that of their fetuses. Such technology would be a logical extension of the telemedicine ecosystem.
Methods
We conducted an observational cross-sectional study via online surveying in the United States. Study participants were recruited using the SurveyMonkey Audience Polling system and responded virtually. In all, the sample consisted of 507 women, aged 18–45 from 45 states, who are expecting to become pregnant in the next five years. Women were asked to identify their willingness to use a wearable ECG device the size of a patch-sized large band-aid on their abdomen. Ten binary or multiple-choice questions were used to gauge population interest and related demographics toward the usage of a wearable ECG device.
Results
Of the 507 participants, 461 (91%) women expressed an acceptance of wearable ECG technology throughout the pregnancy as a mechanism for increased frequency of monitoring of maternal and fetal health outside the hospital. 395 (78%) women demonstrated a willingness to wear devices day and night or at least during sleep and 213 (42%) of the women would spend up to $200 on such a device.
Conclusion
Even though conducted prior to the COVID-19 pandemic, this study clearly indicates a high degree of readiness of prospective pregnant women for telemedicine with continuous health monitoring of the mother-fetus dyad.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Smart wearable electrocardiogram (ECG) devices can enable pregnant women to monitor their health and that of their fetuses, but it was not known how women of child-bearing age perceive the use of remote fetal ECG monitoring technologies throughout the pregnancy period. This study indicates a high degree of readiness of prospective pregnant women for telemedicine with continuous health monitoring of the mother-fetus dyad. |
Introduction
The COVID-19 pandemic has drastically altered the landscape in which healthcare is delivered. Prior to 2019, telemedicine was pitched as the next frontier. However, little was understood about how it would become integrated into modern healthcare delivery. Over the past 2 years, patients have become increasingly accepting of receiving medical care remotely [1]. This represents an exciting social shift that offers enormous opportunities for the improvement of Maternal and Fetal Medicine.
The use of fetal electrocardiogram (ECG) derived from maternal abdominal ECG as a biomarker of fetal well-being offers a prime entry point for the implementation of remote monitoring and telemedicine for this underserved patient population. ECG is a measurement of the electrical activity of the heart. Deviations from normal patterns of the ECG waveform have long been used as a diagnostic tool for pathologies ranging from myocardial infarction to cardiac rhythm disorders to electrolyte abnormalities. While ultrasound-based monitoring of fetal cardiac activity (cardiotocography (CTG)-derived fetal heart rate) remains the mainstay of the intermittent antepartum and continuous intrapartum monitoring of fetal well-being, this technology is fundamentally limited in its signal quality, signal continuity, and the temporal precision of cardiac activity waveform, in particular the beat-to-beat intervals which are used to derive fetal heart rate (FHR) and FHR variability metrics (Frasch 2022; Frasch 2020). ECG patterns are currently being investigated as early biomarkers of poor fetal and postnatal development [2, 3]. Studies indicate that adverse stimuli such as chronic maternal stress can negatively impact lifelong neurodevelopmental trajectories [4]. Current practice is only beginning to use ECG as a source of biomarkers intrapartum and not at all antepartum [5, 6].
The average number of prenatal visits in Europe and the United States is 6 and 11, respectively, with no indication that a higher frequency of prenatal visits results in better neonatal outcomes [7]. This suggests that a higher frequency of intermittent prenatal visits as such does not help improve the management of pregnancy. On the other hand, the prevailing paradigm is that earlier and continually updated information about physiological phenotype provides opportunities for more personalized health care in terms of prevention and early risk assessment. That can be achieved by continuous (or almost continuous) physiological monitoring of maternal and fetal health using ECG technologies. Applying this technology to the in-home setting will expand the intervention window for providers, improving pregnancy outcomes. Mothers would continuously wear ECG devices monitoring both maternal and fetal ECG and its derivatives, such as heart rate (HR) and HR variability metrics, providing instant on-site and remote access to the health of the mother-fetus dyad. The first step in the implementation of such practices is gauging how perceptive prospective and existing mothers would be to the integration of wearable ECG devices in their daily lives.
Methods
To gauge their interest in the use of a wearable maternal–fetal ECG device, we conducted an observational cross-sectional study. To recruit and poll participants, the SurveyMonkey Audience system was used from July 31st to August 1st of 2019, to survey 507 female participants across the United States of the ages 18–45, with annual income brackets of $0–$200,000.
SurveyMonkey is an online survey tool used to collect data from individuals across the US population. A pool of over 2 million people is maintained through an agreement wherein participants agree to take part in a survey, in exchange for SurveyMonkey making a donation of $0.50 to the charity of that individual’s choice. The SurveyMonkey algorithm then randomly assigns participants to surveys in a manner that creates a sample representative of the demographics specified by the investigator. Participants then receive a URL via email from which the survey can be completed on a laptop or mobile device.
Study ethics approach
Each survey participant was first given the option to opt out of the survey (Question 1). Only if agreed to continue, were the subsequent questions shown. Due to the completely anonymous nature of the data collection and the provided right to opt out of the survey or agree to continue, no IRB approval was obtained prior to the survey’s completion. However, after the completion of the survey and prior to publication of the findings, we consulted the UW IRB. It was determined that the approach taken meets the definition of “minor non-compliance” with IRB-approved procedures/UW policies and procedures, because it posed no significant increase in risk or any decrease in benefits to subjects. The IRB ruled that this means that the data collected as part of this research cannot be described as part of a study reviewed by human subject division (IRB). On January 24, 2022, the IRB determined that the corrective actions described in the report are sufficient. No additional actions are required at this time.
Survey structure
This study was conducted under the parameters of a nationally representative sample containing 500 females ranging 18–45 years of age with an annual income range of $0–200,000. Participants were asked a total of 10 questions. We screened the participants by initially asking: “Are you planning to be pregnant in the next 5 years?” If no, the questionnaire was stopped; if yes participants answered four questions to gauge interest in a wearable ECG device as seen in Fig. 1. When asked question four, participants were given a description (Table 1) of a wearable device the size of a “patch-sized large band-aid” worn on the abdomen for at least 8 continuous hours throughout the day or night to help doctors ensure they are in good health during pregnancy. Eight hours was established for two reasons. First, it was deemed an appropriate length of time to reliably collect maternal abdominal ECG that can yield maternal and fetal ECG while accounting for maternal and fetal sleep states [8, 9]. Second, eight hours would fit into the standard sleep schedule and avoid interruptions in data collection. Demographics were then gathered via five additional questions to identify income, age, location, gender, and polling device type distribution among the cohort.

Survey question algorithm
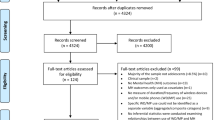
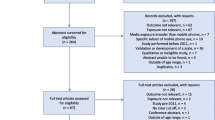
To achieve adequate power to accurately represent the roughly 60 million US females between the ages of 18–45, we determined that 500 participants were needed. In order to gather enough responses for each of the ten questions, SurveyMonkey recruited a total of 527 participants. The response rate among recruited individuals was 96%, with twenty recruited individuals failing to provide a response to all presented questions. The initial screening question had a margin of error of 4.44% due to 507 individuals responding to “planning to become pregnant in the next 5 years”. Questions 2–5 had a margin of error of 6% due to participants choosing not to answer. Questions 6–10 which were used to gather cohort demographics, had a margin of 4.4% as all 507 responded. In total, the data collected using the SurveyMonkey Audience System had a confidence level of 95%.
Results
The cohort represented individuals from forty-five states across the USA, with response density reflecting population densities (Fig. 2).

Geographic representation of surveyed participants. The cohort represented individuals from forty-five states across the USA, with response density reflecting population densities
A 96% response rate (507/527) was achieved because participants were recruited and agreed to complete a survey in principle prior to participation, with no knowledge of the survey’s content. SurveyMonkey then randomly assigned participants to our survey, from the pool of individuals who agreed to partake in any survey, until all questions had a response rate of 250. This led to a total recruitment of 527 individuals, twenty of which did not complete the survey and whose responses could not be included. Participants make up females 18–45 with incomes ranging $0–200,000 from 45 of the 50 states in the US.
As Table 2 summarizes, a large proportion [113 (43.8%)] of participants had already gone through a prior pregnancy. The screening question identified 258 participants, or roughly half of the participants (50.89%) as planning to become pregnant within five years of participating in the study. 121 (46.9%) participants expressed a willingness to wear an ECG device continuously, 81 (31.4%) only while sleeping, or 33 (12.8%) only while awake (Fig. 3). Individuals were also polled on their inclinations to spend money on said device, 105 (44.7%) were willing to spend up to $100 on such a product, and another 98 (41.7%) $100 to $200 (Fig. 3). A subset of 23 (9.79%) participants expressed a willingness to spend up to $300, and an additional (9) 3.83% demonstrated a readiness to spend more than $300 on a wearable ECG device.

Survey findings
Discussion
Five hundred and seven women of childbearing age, the largest population sample surveyed to date for this purpose, provided insight into their attitudes towards wearable ECG devices. Of those 258 participants that affirmed to become pregnant in the next 5 years, the overwhelming majority (235) expressed enthusiasm toward a wearable device for monitoring maternal–fetal health during pregnancy in-home, while asleep, and on the go.
ECG-based monitoring devices for pregnant women can enable deeper analyses and more precise reporting of health status than current ultrasound-based devices. Ultrasound is limited as a diagnostic tool due to the small size and constant motion of the fetus. Ultrasound gives snapshot data points that are highly dependent on human experience and interpretation, unlike ECG which allows for real-time monitoring of the fetus [10].
ECG-based telemedicine does have its limitations. Technical challenges are posed by the internal nature of the fetus as maternal tissue and amniotic fluid can mask and distort signals creating a low signal-to-noise ratio. In addition, the fetal heart rate is 2–3 times faster than that of an adult further complicating signal extraction issues [11].
The introduction of wearable ECG devices may also create psychosocial complications. Pregnant women may experience a heightened awareness of the impact their behavior has on fetal health due to the continuous presence of a monitoring device. This heightened awareness could lead to improved dietary and lifestyle choices. Conversely, it may incur an increased stress response in the mother. There is also potential for the presence of ECG devices to promote increased levels of communication with the prenatal care team and subsequently improve care outcomes. However, there is also the potential for providers to become overwhelmed with inquiries from well-meaning pregnant mothers about the status of their fetus. Our team believes the potential psychosocial complications are far outweighed by the positive impact on the quality of care provided to pregnant mothers.
The findings of this study indicate that the child-bearing aged female population is ready for the integration of wearable continuous ECG monitoring into the modern healthcare model of telemedicine. The time for disruption of the present antiquated maternal–fetal monitoring antepartum has arrived. The required hardware and software technologies have matured and converged with the people’s readiness for telemedicine throughout the antepartum period. ECG-based monitoring devices for pregnant women will allow more robust analyses and more accurate reporting of health status than current ultrasound-based devices.
The strengths of the present study include a large cross-sectional US-wide representative population sampling approach with a response rate over 95% and a margin of error around 4%. The key limitation is that we conducted no piloting and validation of the questions 4 and 5 deployed in our survey. A mitigating circumstance is a fact that the questions were either binary or simple multiple-choice queries leaving little room for interpretation.
In today’s health technology market wearable products that monitor adult health and fitness do exist but are not targeted specifically towards pregnant women. Therefore, currently, no routinely used antepartum monitoring technology exists that provides information on the pregnancy physiology or the health status of the fetus or the pregnant mother. However, excitingly, several companies are pursuing this direction in clinical research settings as the first step toward implementation in routine clinical care Non-wearable products that monitor aspects of fetal health exist in the consumer space. However, such devices all share common pitfalls like low fidelity ultrasound technology, very short-term (seconds to minutes) observations without data recordings, and provide minimal data analytics (if any) value beyond brief entertainment and possibly perilous false reassurance.
At the same time, the cost of hardware components required to build high-quality ECG devices for this purpose has come down to such a level that continuous antepartum monitoring technology is now achievable within the price range identified in the present study. All required software components are also available [3, 12,13,14].
From a physiological viewpoint, a pregnant woman and her unborn baby are intimately connected forming one single physiological system. Consequently, important information about their joint well-being is lost when they are not monitored together [15]. With one recent exception, all current devices use periodic ultrasound-based monitoring which is less precise than ECG-based monitoring and cannot provide the continuous monitoring (during maternal sleep for example) that is possible with ECG-based wearable devices [6].
References
Mann DM, Chen J, Chunara R et al (2020) COVID-19 transforms health care through telemedicine: evidence from the field. J Am Med Inform Assoc 27:1132–1135. https://doi.org/10.1093/jamia/ocaa072
Frasch MG (2020) Letter to the Editor: Mind the gap: epistemology of heart rate variability. Am J Physiol Regul Integr Comp Physiol 319:R343–R344. https://doi.org/10.1152/ajpregu.00183.2020
Sarkar P, Lobmaier S, Fabre B et al (2021) Detection of maternal and fetal stress from the electrocardiogram with self-supervised representation learning. Sci Rep 11:24146. https://doi.org/10.1038/s41598-021-03376-8
Lobmaier SM, Müller A, Zelgert C et al (2020) Fetal heart rate variability responsiveness to maternal stress, non-invasively detected from maternal transabdominal ECG. Arch Gynecol Obstet 301:405–414. https://doi.org/10.1007/s00404-019-05390-8
Tamber KK, Hayes DJL, Carey SJ et al (2020) A systematic scoping review to identify the design and assess the performance of devices for antenatal continuous fetal monitoring. PLoS ONE 15:e0242983. https://doi.org/10.1371/journal.pone.0242983
Mhajna M, Schwartz N, Levit-Rosen L et al (2020) Wireless, remote solution for home fetal and maternal heart rate monitoring. Am J Obstet Gynecol MFM. https://doi.org/10.1016/j.ajogmf.2020.100101
Carter EB, Tuuli MG, Caughey AB et al (2016) Number of prenatal visits and pregnancy outcomes in low-risk women. J Perinatol 36:178–181. https://doi.org/10.1038/jp.2015.183
Zavala JH, Ecklund-Flores L, Myers MM, Fifer WP (2020) Assessment of autonomic function in the late term fetus: the effects of sex and state. Dev Psychobiol 62:224–231. https://doi.org/10.1002/dev.21865
DiPietro JA, Raghunathan RS, Wu H-T et al (2021) Fetal heart rate during maternal sleep. Dev Psychobiol 63:945–959. https://doi.org/10.1002/dev.22118
Lempersz C, van Laar JO, Clur S-AB et al (2020) The standardized 12-lead fetal electrocardiogram of the healthy fetus in mid-pregnancy: a cross-sectional study. PLoS ONE 15:e0232606. https://doi.org/10.1371/journal.pone.0232606
Verdurmen KMJ, Lempersz C, Vullings R et al (2016) Normal ranges for fetal electrocardiogram values for the healthy fetus of 18–24 weeks of gestation: a prospective cohort study. BMC Pregnancy Childbirth 16:227. https://doi.org/10.1186/s12884-016-1021-x
Su L, Wu H-T (2017) Extract fetal ECG from single-lead abdominal ECG by de-shape short time Fourier transform and nonlocal median. Front Appl Math Stat 3:2. https://doi.org/10.3389/fams.2017.00002
Frasch MG (2020) Heart rate variability code: does it exist and can we hack it? https://doi.org/10.48550/arXiv.2001.08264
Frasch MG (2022) Comprehensive HRV estimation pipeline in Python using Neurokit2: application to sleep physiology. MethodsX
Frasch MG, Lobmaier SM, Stampalija T et al (2020) Non-invasive biomarkers of fetal brain development reflecting prenatal stress: an integrative multi-scale multi-species perspective on data collection and analysis. Neurosci Biobehav Rev 117:165–183. https://doi.org/10.1016/j.neubiorev.2018.05.026
Acknowledgements
The authors gratefully acknowledge the assistance of D. Levitan and Y. Kimelfeld during the survey design.
Funding
The study was funded by Fetal Precision LLC.
Author information
Authors and Affiliations
Contributions
MGF, LY and SS conceived and carried out the study. MGF and CW did the data analysis. MGF wrote the initial draft of the manuscript. CW and MGF finalized the manuscript. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
The study was conducted as part of a research project by Fetal Precision LLC. The company has since dissolved, and the findings have been open-sourced. M. G. Frasch has patents on aECG (WO2018160890) and EEG technologies for fetal monitoring (US9215999). The authors declare that the research was conducted in the absence of any other commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical approval
Each survey participant was first given the option to opt out of the survey (Question 1). Only if agreed to continue, were the subsequent questions shown. Due to the completely anonymous nature of the data collection and the provided right to opt out of the survey or agree to continue, no IRB approval was obtained prior to the survey’s completion. However, after the completion of the survey and prior to publication of the findings, we consulted the UW IRB. It was determined that the approach taken meets the definition of “minor non-compliance” with IRB approved procedures/UW policies and procedures, because it posed no significant increase in risk or any decrease in benefits to subjects. The IRB ruled that this means that the data collected as part of this research cannot be described as part of a study reviewed by human subject division (IRB). On January 24, 2022, the IRB determined that the corrective actions described in the report are sufficient. No additional actions are required at this time.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wakefield, C., Yao, L., Self, S. et al. Wearable technology for health monitoring during pregnancy: an observational cross-sectional survey study. Arch Gynecol Obstet 308, 73–78 (2023). https://doi.org/10.1007/s00404-022-06705-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-022-06705-y