
Abstract
Purpose
There is relatively little information on episiotomies in the context of restricted episiotomy use. This study sought to examine maternal and neonatal injuries with restricted episiotomy use.
Methods
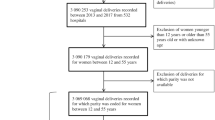
We performed a retrospective database analysis of vaginal deliveries at a tertiary care maternity hospital from June 2010 to June 2015. Maternal injuries (third- or fourth-degree lacerations) and neonatal injuries (birth trauma) were identified through the International Classification of Diseases, Ninth Revision, codes. Vaginal deliveries were classified as spontaneous, vacuum-assisted, or forceps-assisted. The associations between episiotomy and maternal and neonatal injuries were examined with stratification by parity, type of vaginal delivery, and type of episiotomy (midline or mediolateral). Adjusted-odds’ ratios were calculated for maternal and neonatal injuries using a multiple logistic regression model to adjust for potential confounders.
Results
22,800 deliveries occurred during the study interval involving 23,016 neonates. The episiotomy rate was 6.7 % overall and 22.9 % in operative vaginal deliveries. Episiotomies, both midline and mediolateral, were associated with increased risks of maternal and neonatal injuries regardless of parity (p < 0.0001). Upon stratification by the type of delivery, the association with maternal injury remained only for spontaneous vaginal deliveries (p < 0.0001). Adjusted-odds’ ratios demonstrated a continued association between episiotomy and maternal [aOR 1.67 (1.39–2.05)] and neonatal injuries [aOR 1.43 (1.17–1.73)].
Conclusion
Episiotomy continues to be associated with increased third- and fourth-degree lacerations with restricted use, particularly in spontaneous vaginal deliveries.
Similar content being viewed by others


References
Weber AM, Meyn L (2002) Episiotomy use in the United States, 1979–1997. Obstet Gynecol 100:1177–1182
American College of Obstetricians and Gynecologists (2006) Episiotomy. Practice bulletin No. 71. Obstet Gynecol 107:957–962
Dudding TC, Vaizey CJ, Kamm MA (2008) Obstetric anal sphincter injury: incidence, risk factors, and management. Ann Surg 247:224–237
Edozien LC, Gurol-Urganci I, Cromwell DA, Adams EJ, Richmond DH, Mahmood TA et al (2014) Impact of third- and fourth-degree perineal tears at first birth on subsequent pregnancy outcomes: a cohort study. BJOG 121:1695–1704
Friedman AM, Ananth CV, Prendergast E, D’Alton ME, Wright JD (2015) Variation in and factors associated with use of episiotomy. JAMA 313:197–199
Landy HJ, Laughon SK, Bailit JL, Kominiarek MA, Gonzalez-Quintero VH, Ramirez M et al (2011) Characteristics associated with severe perineal and cervical lacerations during vaginal delivery. Obstet Gynecol 117:627–635
Steiner N, Weintraub AY, Wiznitzer A, Sergienko R, Sheiner E (2012) Episiotomy: the final cut? Arch Gynecol Obstet 286:1369–1373
Raisanen S, Cartwright R, Gissler M, Kramer MR, Laine K, Jouhki M et al (2013) Changing associations of episiotomy and anal sphincter injury across risk strata: results of a population-based register study in Finland. BMJ Open 3:e003216
Raisanen S, Vehvilainen-Julkunen K, Gissler M, Heinonen S (2012) Hospital-based lateral episiotomy and obstetric anal sphincter injury rates: a retrospective population-based register study. Am J Obstet Gynecol 206:347.e1–347.e6
de Vogel J, van der Leeuw-van Beek A, Gietelink D, Vujkovic M, de Leeuw JW, van Bavel J et al (2012) The effect of a mediolateral episiotomy during operative vaginal delivery on the risk of developing obstetrical anal sphincter injuries. Am J Obstet Gynecol 206:404.e1–404.e5
Revicky V, Nirmal D, Mukhopadhyay S, Morris EP, Nieto JJ (2010) Could a mediolateral episiotomy prevent obstetric anal sphincter injury? Eur J Obstet Gynecol Reprod Biol 150:142–146
Carroli G, Mignini L (2012) Episiotomy for vaginal birth. Cochrane Database Syst Rev Issue 1 Art No:CD000081. doi:10.1002/14651858.CD000081.pub2
Sagi-Dain L, Sagi S (2015) Morbidity associated with episiotomy in vacuum delivery: a systematic review and meta-analysis. BJOG 122:1073–1081
Macleod M, Strachan B, Bahl R, Howarth L, Goyder K, Van de Venne M et al (2008) A prospective cohort study of maternal and neonatal morbidity in relation to use of episiotomy at operative vaginal delivery. BJOG 115:1688–1694
Kudish B, Blackwell S, Mcneeley SG, Bujold E, Kruger M, Hendrix SL et al (2006) Operative vaginal delivery and midline episiotomy: a bad combination for the perineum. Am J Obstet Gynecol 195:749–754
Davies-Tuck M, Biro M, Mockler J, Stewart L, Wallace EM, East C (2015) Maternal Asian ethnicity and the risk of anal sphincter injury. Acta Obstet Gynecol Scand 94:308–315
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
No funding source was utilized for this study.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required. This study received IRB exemption from the Hawaii Pacific Health Research Institute.
Appendix: International Classification of Diseases-9 (ICD-9) codes used to identify maternal and neonatal injuries
Appendix: International Classification of Diseases-9 (ICD-9) codes used to identify maternal and neonatal injuries
ICD-9 | Code description | Corresponding ICD-10 |
|---|---|---|
Maternal injury | ||
664.20 | Third-degree perineal laceration unspecified as to episode of care in pregnancy | O70.2 |
664.21 | Third-degree perineal laceration with delivery | O70.2 |
664.30 | Fourth-degree perineal laceration unspecified as to episode of care in pregnancy | O70.3 |
664.31 | Fourth-degree perineal laceration with delivery | O70.3 |
Neonatal injury | ||
767.0 | Subdural and cerebral hemorrhage, birth trauma | P10.0; P10.1; P10.4 |
767.11 | Epicranial subaponeurotic hemorrhage | P12.2 |
767.19 | Other birth injuries to scalp | P12.0; P12.89 |
767.2 | Fracture of clavicle, birth trauma | P13.4 |
767.3 | Other injuries to skeleton, birth trauma | P13.0; P13.2; P13.3; P13.8 |
767.5 | Facial nerve injury, birth trauma | P11.3 |
767.6 | Injury to brachial plexus, birth trauma | P14.0; P14.1; P14.3 |
767.7 | Other cranial and peripheral nerve injuries, birth trauma | P11.4; P14.2; P14.8 |
767.8 | Other specified birth trauma | P15.0; P15.1; P15.2; P15.3; P15.5; P15.8 |
767.9 | Birth trauma, unspecified | P15.9 |
Rights and permissions
About this article

Cite this article
Yamasato, K., Kimata, C., Huegel, B. et al. Restricted episiotomy use and maternal and neonatal injuries: a retrospective cohort study. Arch Gynecol Obstet 294, 1189–1194 (2016). https://doi.org/10.1007/s00404-016-4154-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-016-4154-2