
Abstract
Background
There is significant increase in proportion of cases with previous cesarean delivery requiring obstetric care. The available literature fails to provide uniform opinion on each woman’s characteristics to identify risk of uterine rupture while planning trial of labor after cesarean.
Objective
To study the association of abnormal lower uterine segment with some of the present and previous obstetric variables including patient characteristics and surgical techniques at previous cesarean operation.
Materials and methods
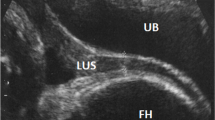
Consenting consecutive 96 post-cesarean singleton pregnancies admitting after 36 weeks gestation at the same facility from July 2011 to December 2012 for repeat cesarean, were studied. Only the cases with cephalic presentation and vertex as presenting part, having no placenta previa, polyhydramnios, uterine anomaly or fibroid and those who had previous one lower segment cesarean were recruited. Based on the intra-operative finding the lower uterine segment (LUS) was categorized into those having a normal and abnormal (grades 2–4) LUS. Sonographic assessment of LUS thickness and any abnormalities if any were noted. The findings of abnormal LUS (direct observation at surgery and sonographic impression within a week before surgery) were looked for association with some of the present and previous obstetric variables including patient characteristics and surgical techniques at previous cesarean operation using Student t, Chi square or Fisher’s exact test for analysis as appropriate. Receiver operating curve analysis was used to determine the optimal cut off value for prediction of LUS integrity by ultrasound.
Results
Of the women recruited for the study, 36 were admitted in early labor and ultrasound evaluation of LUS was performed in 48 of the remaining 60 women admitted antenatal for elective cesarean delivery. There were 38 abnormal LUS (39.6 %) with 22 of them (57.9 %) graded as ‘thinned out LUS’. The incidence of scar dehiscence (grade 3, cases 5) was 5.2 % of 96 cases and there were no cases of scar rupture. Proportion of cases with abnormal LUS was significantly high when primary cesarean was done in preterm (p = 0.02); it was a single layer uterine closure (p = 0.02), and inter-cesarean interval was 54 months (p = 0.01). Abnormal LUS was also seen to be associated with maternal age beyond 35 years (p = 0.2), when cesarean was performed in labor (p = 0.5), following 18 h of rupture of membranes (p = 0.75), for a baby weight more than 3 kg (p = 0.4), and different suture materials (polyglactin 910 and chromic catgut) were used to close uterus at primary cesarean delivery (p = 0.1), and also if they had post-partum fever (p = 0.3). Ultrasound measurement of LUS by abdominal scan correlated with the intra-operative LUS grading and a thickness of more than 3.2 mm within a week before delivery and was seen to be the safe cut off above which most of the women had a normal LUS (sensitivity 92.3 %, specificity 81.1 %).
Conclusion
Factors at primary cesarean operation significantly influence the state of LUS at term in subsequent pregnancy .

Similar content being viewed by others


References
Stanton CK, Holtz SA (2006) Levels and trends in cesarean birth in the developing world. Stud Fam Plan 37:41–48
Guise JM, McDonagh MS, Osterweil P, Nygren P, Chan BK, Helfand M (2004) Systematic review of the incidence and consequences of uterine rupture in women with previous caesarean section. BMJ 329:19–25
Landon MB, Hauth JC, Leveno KJ, Spong CY, Leindecker S, Varner MW et al (2004) Maternal and perinatal outcomes associated with a trial of labor after prior cesarean delivery. N Engl J Med 351:2581–2589
Todman D (2007) A history of caesarean section: from ancient world to modern era. Aust N Z J Obstet Gynaecol 47:357–361
Dodd JM, Anderson ER, Gates S. (2008) Surgical techniques for uterine incision and uterine closure at the time of caesarean section. Cochrane database of Systematic reviews; Issue 3. Art No: CD 004732
Bujold E, Bujold C, Hamilton EF, Harel F, Gauthier RJ (2002) The impact of single layer or double layer closure on uterine rupture. Am J Obstet Gynecol 186:1326–1330
Gyamfi C, Juhasz G, Gyamfi P, Blumenfeld Y, Stone JL (2006) Single- versus double-layer uterine incision closure and uterine rupture. J Matern Fetal Neonatal Med 19:639–643
Bujold E, Goyet M, Marcoux S, Brassard N, Cormier B, Hamilton E et al (2010) The role of uterine closure in the risk of uterine rupture. Obstet Gynecol 116:43–50
Durnwald C, Mercer B (2003) Uterine rupture, perioperative and perinatal morbidity after single-layer and double-layer closure at cesarean delivery. Am J Obstet Gynecol 189:925–929
Tucker JM, Hauth JC, Hodgkins P, Owen J, Winkler CL (1993) Trial of labor after a one- or two-layer closure of a low transverse uterine incision. Am J Obstet Gynecol 168:545–546
Kok N, Wiersma IC, Opmeer BC, de Graaf IM, Mol BW, Pajkrt E (2013) Sonographic measurement of lower uterine segment thickness to predict uterine rupture during a trial of labour in women with previous Cesarean section: a meta-analysis. Ultrasound Obstet Gynecol 42:132–139
Jastrow N, Chaillet N, Roberge S, Morency AM, Lacasse Y, Bujold E (2010) Sonographic lower uterine segment thickness and risk of uterine scar defect: a systematic review. J Obstet Gynaecol Can 32:321–327
Kushtagi P, Garepalli S (2011) Sonographic assessment of lower uterine segment at term in women with previous cesarean delivery. Arch Gynecol Obstet 283:455–459
Quereshi B, Inafku K, Oshima K, Masamoto H, Koj K (1997) Ultrasonographic evaluation of lower uterine segment to predict the integrity and quality of cesarean scar during pregnancy: a prospective study. Tohuku J Exp Med 183:55–65
Bérubé L, Arial M, Gagnon G, Brassard N, Boutin A, Bujold E (2011) Factors associated with lower uterine segment thickness near term in women with previous caesarean section. J Obstet Gynaecol Can 33:581–587
Kaczmarczyk M, Sparén P, Terry P, Cnattingius S (2010) Risk factors for uterine rupture and neonatal consequences of uterine rupture: a population-based study of successive pregnancies in Sweden. BJOG 117:809–820
Friedman EA, Sachtleben MR (1965) Relation of maternal age to the course of labor. Am J Obstet Gynecol 91:915–924
Shipp TD, Zelop C, Repke JT, Cohen A, Caughey AB, Lieberman E (2002) The association of maternal age and symptomatic uterine rupture during a trial of labor after prior cesarean delivery. Obstet Gynecol 99:585–588
Shipp TD, Zelop CM, Repke JT, Cohen A, Lieberman E (2001) Interdelivery interval and risk of symptomatic uterine rupture. Obstet Gynecol 97:175–177
Bujold E, Gauthier RJ (2010) Risk of uterine rupture associated with an interdelivery interval between 18 and 24 months. Obstet Gynecol 115:1003–1006
Chapman SJ, Owen J, Hauth JC (1997) One – versus two – layer closure of a low transverse cesarean: the next pregnancy. Obstet Gynecol 89:16–18
Roberge S, Chaillet N, Boutin A, Moore L, Jastrow N, Brassard N et al (2011) Single versus double-layer closure of the hysterotomy incision during cesarean delivery and risk of uterine rupture. Int J Gynaecol Obstet 115:5–10
Macones GA, Peipert J, Nelson DB, Odibo A, Stevens EJ, Stamilio DM et al (2005) Maternal complications with vaginal birth after cesarean delivery: a multicenter study. Am J Obstet Gynecol 193:1656–1662
Hammoud A, Hendler I, Gauthier RJ, Berman S, Sansregret A, Bujold E (2004) The effect of gestational age on trial of labor after cesarean section. J Matern Fetal Neonatal Med 15:202–206
Kiran TS, Chui YK, Bethel J, Bhal PS (2006) Is gestational age an independent variable affecting uterine scar rupture rates? Eur J Obstet Gynecol Reprod Biol 126:68–71
Craver Pryor E, Mertz HL, Beaver BW, Koontz G, Martinez-Borges A, Smith JG et al (2007) Intrapartum predictors of uterine rupture. Am J Perinatol 24:317–321
Zelop CM, Shipp TD, Repke JT, Cohen A, Lieberman E (2001) Outcomes of trial of labor following previous cesarean delivery among women with fetuses weighing >4000 g. Am J Obstet Gynecol 185:903–905
Sciscione AC, Landon MB, Leveno KJ, Spong CY, Macpherson C, Varner MW et al (2008) Previous preterm cesarean delivery and risk of subsequent uterine rupture. Obstet Gynecol 111:648–653
Myerscough PR (1998) Uterine action in labour: normal and abnormal. In: Munro Kerr’s operative obstetrics, 10th edn. Bailliere Tindall, London, p 39
Algert CS, Morris JM, Simpson JM, Ford JB, Roberts CL (2008) Labor before a primary cesarean delivery: reduced risk of uterine rupture in a subsequent trial of labor for vaginal birth after cesarean. Obstet Gynecol 112:1061–1066
Uldbjerg N, Ekman G, Malmström A, Sporrong B, Ulmsten U, Wingerup L (1981) Biochemical and morphological changes of human cervix after local application of prostaglandin E2 in pregnancy. Lancet 1:267–268
Bujold E, Jastrow N, Simoneau J, Brunet S, Gauthier RJ (2009) Prediction of complete uterine rupture by sonographic evaluation of lower uterine segment. Am J Obstet Gynecol 201:320–326
Sen S, Malik S, Salhan S (2004) Ultrasonographic evaluation of lower uterine segment thickness in patients of previous cesarean section. Int J Gynaecol Obstet 87:215–219
Conflict of interest
Nil to declare. The study was not sponsored by any agency/organization. The Journal can request the primary data for review at any time.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Brahmalakshmy, B.L., Kushtagi, P. Variables influencing the integrity of lower uterine segment in post-cesarean pregnancy. Arch Gynecol Obstet 291, 755–762 (2015). https://doi.org/10.1007/s00404-014-3455-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-014-3455-6