
Abstract
Objective
The main interest of this study was to assess the rate of intraoperative and perioperative complications of laparoscopic supracervical hysterectomy (LASH) in a teaching hospital.
Methods
A retrospective analysis of 1,584 laparoscopic assisted hysterectomies between 2005 and 2010 by different surgeons.
Results
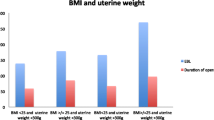
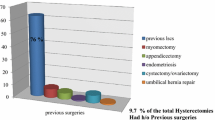
In 2,577 patients undergoing simple hysterectomy, an indication for LASH was present in 1,584 cases. Indications were uterine myomas (71.6%), dysfunctional uterine bleeding (12.6%), suspicion of adenomyosis uteri (8.9%), descensus uteri (2.8%), dysmenorrhea (2.8%), hysterectomy on demand (1.2%) and benign hyperplasia of the endometrium (0.2%). Mean duration of the procedure was 76.5 ± 33.4 min (95% CI, ±1.66). The average age of patients was 45.9 ± 5.4 years (95% CI, ±0.27). Mean body mass index (BMI) was 25.3 ± 4.9 (95% CI, ±0.24). Adhesiolysis due to earlier surgery had to be performed in 190 (12%) cases. The total complication rate was 1.07%. The total conversion rate to laparotomy was 0.88%. The rate of conversion after laparoscopic assessment of the situs was 0.57%. In five cases, conversion to laparotomy was necessary due to intraoperative complications (0.32%). On the whole, six bleedings (0.38%), four bladder injuries (0.25%), three intestinal injuries (0.19%), one ureter injury (0.06%), one injury of the epigastric vein (0.06%) and two omental incarcerations (0.13%) occurred.
Conclusion
In this retrospective analysis, the rate of complications for LASH was very low in a hospital of standard care and residency. LASH has to be considered as a minimally invasive method with a low perioperative morbidity to treat benign uterine pathologies even in a teaching setting and should therefore be the method of choice if the cervix can be preserved.
Similar content being viewed by others

References
Roumm AR, Pizzi L, Goldfarb NI, Cohn H (2005) Department of health policy, minimally invasive: minimally reimbursed? An examination of six laparoscopic surgical procedures. USA Surg Innov 12(3):261–287
Semm K (1991) Hysterectomy via laparotomy or pelviscopy. A new CASH method without colpotomy. Geburtshilfe Frauenheilkd 51(12):996–1003
El-Mowafi D, Madkour W, Lall C, Wenger JM (2004) Laparoscopic supracervical hysterectomy versus laparoscopic-assisted vaginal hysterectomy. J Am Assoc Gynecol Laparosc 11(2):175–180
Donnez J, Nisolle M (1993) Laparoscopic supracervical (subtotal) hysterectomy (LASH). J Gynecol Surg 9(2):91–94
Sarmini OR, Lefholz K, Froeschke HP (2005) A comparison of laparoscopic supracervical hysterectomy and total abdominal hysterectomy outcomes. J Minim Invasive Gynecol 12(2):121–124
Hoffman CP, Kennedy J, Borschel L, Burchette R, Kidd A (2005) Laparoscopic hysterectomy: the Kaiser Permanente San Diego experience. J Minim Invasive Gynecol 12(1):16–24
Lyons TL (2000) Laparoscopic supracervical hysterectomy. Obstet Gynecol Clin North Am 27(2):441–450
Milad MP, Morrison K, Sokol A, Miller D, Kirkpatrick L (2001) A comparison of laparoscopic supracervical hysterectomy versus laparoscopically assisted vaginal hysterectomy. Surg Endosc 15(3):286–288
Kondo W, Bourdel N, Tamburro S, Cavoli D, Jardon K, Rabischong B, Botchorishvili R, Pouly J, Mage G, Canis M (2011) Complications after surgery for deeply infiltrating pelvic endometriosis. BJOG 118(3):292–298. doi:10.1111/j.1471-0528.2010.02774.x
Bojahr B, Raatz D, Schonleber G, Abri C, Ohlinger R (2006) Perioperative complication rate in 1,706 patients after a standardized laparoscopic supracervical hysterectomy technique. J Minim Invasive Gynecol 13(3):183–189
Kolmorgen K (1998) Laparoscopy complications in previously operated patients. Zentralbl Gynakol 120(4):191–194
Ellis H, Moran BJ, Thompson JN, Parker MC, Wilson MS, Menzies D, McGuire A, Lower AM, Hawthorn RJ, O’Brien F, Buchan S, Crowe AM (1999) Adhesion-related hospital readmissions after abdominal and pelvic surgery: a retrospective cohort study. Lancet 353(9163):1476–1480
Léonard F, Fotso A, Borghese B, Chopin N, Foulot H, Chapron C (2007) Ureteral complications from laparoscopic hysterectomy indicated for benign uterine pathologies: a 13-year experience in a continuous series of 1,300 patients. Hum Reprod 22(7):2006–2011
Bojahr B, Tchartchian G, Ohlinger R (2009) Laparoscopic supracervical hysterectomy: a retrospective analysis of 1,000 cases. JSLS 13(2):129–134
Donnez O, Jadoul P, Squifflet J, Donnez J (2009) A series of 3,190 laparoscopic hysterectomies for benign disease from 1990 to 2006: evaluation of complications compared with vaginal and abdominal procedures. BJOG 116(4):492–500
Donnez O, Donnez J (2010) A series of 400 laparoscopic hysterectomies for benign disease: a single centre, single surgeon prospective study of complications confirming previous retrospective study. BJOG 117(6):752–755
Liu CY (1992) Laparoscopic hysterectomy. A review of 72 cases. J Reprod Med 37(4):351–354
Salfelder A, Lueken RP, Bormann C et al (2003) Die suprazervikale Hysterektomie in neuem Licht. Wiederentdeckung als minimalinvasive Methode. Frauenarzt 44:1071–1075
Conflict of interest
We declare that we have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Grosse-Drieling, D., Schlutius, J.C., Altgassen, C. et al. Laparoscopic supracervical hysterectomy (LASH), a retrospective study of 1,584 cases regarding intra- and perioperative complications. Arch Gynecol Obstet 285, 1391–1396 (2012). https://doi.org/10.1007/s00404-011-2170-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-011-2170-9