
Abstract
Introduction
Chronic exertional compartment syndrome (CECS) is a common injury in young athletes, causing pain in the involved leg compartment during strenuous exercise. The gold standard treatment is fasciotomy, but most of the reports on its effectiveness include relatively small cohorts and relatively short follow-up periods. This study reports the long-term results of a large cohort of young athletes who underwent single-incision fasciotomy for CECS.
Materials and methods
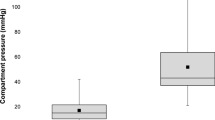
This a retrospective case-series study. All patients treated by fasciotomies performed for CECS between 2007 and 2011, in a tertiary medical institution. CECS was diagnosed following history taking and clinical evaluation, and confirmed by compartment pressure measurements. Ninety-five legs that underwent single-incision subcutaneous fasciotomy were included. Data on the numerical analog scale (NAS), Tegner activity score, and quality-of-life (QOL) as measured via the short form-12 (SF-12) were retrieved from all patients preoperatively and at the end of follow-up.
Results
The average time to diagnosis was 22 months and the mean follow-up was 50.1 months. Sixty-three legs underwent anterior compartment fasciotomy (an additional 30 legs also underwent lateral compartment release), and two legs underwent lateral and peroneal compartment releases. The average change in Tegner score was an improvement of 14.6 points. Similarly, the patients reported a significant improvement in the SF-12 and NAS scores. Satisfaction rates were high (average 75.5 %). The main complications were wound infection (2 patients) and nerve injuries (4 patients). Eight patients had recurrence.
Conclusion
Single-incision fasciotomy leads to long-term improvement in the activity level and QOL of patients with CECS.






Similar content being viewed by others


References
Davis DE, Raikin S, Garras DN, Vitanzo P, Labrador H, Espandar R (2013) Characteristics of patients with chronic exertional compartment syndrome. Foot Ankle Int 34:1349–1354
Wilder RP, Magrum E (2010) Exertional compartment syndrome. Clin Sports Med 29:429–435
Canale S (1998) Campbell’s operative orthopaedics. Elsevier, Philadelphia
Frontera W (2002) Essentials of physical medicine and rehabilitation. Hanley and Belfus, Canada
Brennan FH Jr, Kane SF (2003) Diagnosis, treatment options, and rehabilitation of chronic lower leg exertional compartment syndrome. Curr Sports Med Rep 2:247–250
Dunn JC, Waterman BR (2014) Chronic exertional compartment syndrome of the leg in the military. Clin Sports Med 33:693–705
Fraipont MJ, Adamson GJ (2003) Chronic exertional compartment syndrome. J Am Acad Orthop Surg 11:268–276
Pedowitz RA, Hargens AR, Mubarak SJ, Gershuni DH (1990) Modified criteria for the objective diagnosis of chronic compartment syndrome of the leg. Am J Sports Med 18:35–40
Tucker AK (2010) Chronic exertional compartment syndrome of the leg. Curr Rev Musculoskelet Med 3:32–37
Rom E, Tenenbaum S, Chechick O, Burstein G, Amit Y, Thein R (2013) Chronic exertional compartment syndrome. Harefuah 152:608–611
Wittstein J, Moorman CT 3rd, Levin LS (2010) Endoscopic compartment release for chronic exertional compartment syndrome: surgical technique and results. Am J Sports Med 38:1661–1666
Verleisdonk EJ, Schmitz RF, van der Werken C (2004) Long-term results of fasciotomy of the anterior compartment in patients with exercise-induced pain in the lower leg. Int J Sports Med 25:224–229
Cook S, Bruce G (2002) Fasciotomy for chronic compartment syndrome in the lower limb. ANZ J Surg 72:720–723
DeLee JC et al (2003) DeLee and Drez’s orthopaedic sports medicine. Saunders, Philadelphia
Slimmon D, Bennell K, Brukner P, Crossley K, Bell SN (2002) Long-term outcome of fasciotomy with partial fasciectomy for chronic exertional compartment syndrome of the lower leg. Am J Sports Med 30:581–588
Campano D, Robaina JA, Kusnezov N, Dunn JC, Waterman BR (2016) Surgical management for chronic exertional compartment syndrome of the leg: a systematic review of the literature. Arthroscopy 32(7):1478–1486
Lysholm J, Tegner Y (2007) Knee injury rating scales. Acta Orthop 78:445–453
Tegner Y, Lysholm J (1985) Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res 198:43–49
Ware J Jr, Kosinski M, Keller SD (1996) A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care 34:220–233
Amir M, Lewin-Epstein N, Becker G, Buskila D (2002) Psychometric properties of the SF-12 (Hebrew version) in a primary care population in Israel. Med Care 40:918–928
McCaffery M, Beebe A et al (1989) Pain: clinical manual for nursing practice. Mosby, St. Louis
Detmer DE, Sharpe K, Sufit RL, Girdley FM (1985) Chronic compartment syndrome: diagnosis, management, and outcomes. Am J Sports Med 13:162–170
Howard JL, Mohtadi NG, Wiley JP (2000) Evaluation of outcomes in patients following surgical treatment of chronic exertional compartment syndrome in the leg. Clin J Sport Med 10:176–184
Rorabeck CH, Bourne RB, Fowler PJ (1983) The surgical treatment of exertional compartment syndrome in athletes. J Bone Jt Surg Am 65:1245–1251
Schepsis AA, Martini D, Corbett M (1993) Surgical management of exertional compartment syndrome of the lower leg. Long-term followup. Am J Sports Med 21:811–817 (discussion 817)
Raikin SM, Rapuri VR, Vitanzo P (2005) Bilateral simultaneous fasciotomy for chronic exertional compartment syndrome. Foot Ankle Int 26:1007–1011
Finestone AS, Noff M, Nassar Y, Moshe S, Agar G, Tamir E (2014) Management of chronic exertional compartment syndrome and fascial hernias in the anterior lower leg with the forefoot rise test and limited fasciotomy. Foot Ankle Int 35:285–292
Packer JD, Day MS, Nguyen JT, Hobart SJ, Hannafin JA, Metzl JD (2013) Functional outcomes and patient satisfaction after fasciotomy for chronic exertional compartment syndrome. Am J Sports Med 41:430–436
McCallum JR, Cook JB, Hines AC, Shaha JS, Jex JW, Orchowski JR (2014) Return to duty after elective fasciotomy for chronic exertional compartment syndrome. Foot Ankle Int 35:871–875
Bramante C, Gandolfo L, Bosco V (2008) Minimally invasive fasciotomy in the treatment of chronic exertional anterior compartment syndrome of the leg: personal technique. Chir Ital 60:711–715
Sebik A, Dogan A (2008) A technique for arthroscopic fasciotomy for the chronic exertional tibialis anterior compartment syndrome. Knee Surg Sports Traumatol Arthrosc 16:531–534
Lohrer H, Nauck T (2007) Endoscopically assisted release for exertional compartment syndromes of the lower leg. Arch Orthop Trauma Surg 127:827–834
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Additional information
M. Drexler and T. F. Rutenberg contributed equally to this work.
Rights and permissions
About this article

Cite this article
Drexler, M., Rutenberg, T.F., Rozen, N. et al. Single minimal incision fasciotomy for the treatment of chronic exertional compartment syndrome: outcomes and complications. Arch Orthop Trauma Surg 137, 73–79 (2017). https://doi.org/10.1007/s00402-016-2569-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-016-2569-7