
Abstract
Study design
Retrospective case series.
Objective
To analyze the causes of conversion to open for the surgical treatment of lumbar disc herniation with use of full endoscopic (FE) technique, and prophylaxis of conversion to open also proposed.
Method
50 patients with lumbar disc herniation underwent discectomy using unilateral portal FE interlaminar approach collected from August 2008 to August 2010. All FE operations were performed under general anesthesia and endotracheal intubation. According to the level incision of the ligament flavum, the starting point of nerve root at the dura under endoscopic view was classified as: Type I (starting point of the nerve root was higher than the incision) and Type II (the starting point of nerve root was lower than the incision). The causes and effective prophylactic measurements for cases of conversion to open were analyzed.
Results
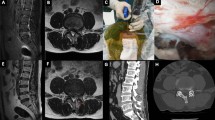
There were 47 cases classified as Type I for a rate of 94 %, and Type II in 3 cases for a rate of 6 %. Five cases were converted to open surgery, and the conversion rate was 10 %. There were three males and two females with a mean age of 36.2 (29–44) years, the average duration of symptoms was 58.4 (35–105) days. The level was L5–S1 in four cases and L4–5 in one, lateral extrusion in three cases, paracentral extrusion in one, and sequestration in one. Leg pain resolved in three cases and improved in two after open surgery. Of five cases of conversion to open, misplacement of the working portal occurred in one case (Type I). Difficult dissection of nerve root and hemostasis resulting in open conversion occurred in one case (Type II); this patient sustained a dural injury. The nerve root could not be exposed in three cases (Type II), the FE changed to open finally. During the open procedure with Type II, we found that the location of origin of the nerve root was caudal to the inferior laminar edge. Therefore, partial removal of bony structures along lateral recess was necessary in order to visualize the nerve root.
Conclusion
Misplacement of working portal during the exposure of the ligament flavum and difficulty in indentifying anatomy are potential causes for conversion to open in the initial adoption of FE technique. However, uncommon conditions such as variation of the nerve root origin can also result in conversion to open in experienced hands. Endoscopic experience, proper patient selection and specific radiographic examination are needed to obtain optimal outcomes using a full endoscopic technique for microdiscectomies.





Similar content being viewed by others


References
Ruetten S, Komp M, Merk H, Godolias G (2007) Use of newly developed instruments and endoscopes: full-endoscopic resection of lumbar disc herniations via the interlaminar and lateral transforaminal approach. J Neurosurg Spine 6:521–530
Kambin P, Casey K, O’Brien E, Zhou L (1996) Transforaminal arthroscopic decompression of the lateral recess stenosis. J Neurosurg 3:462–467
Kambin P, O’Brien E, Zhou L, Schaffer JL (1998) Arthroscopic microdiscectomy and selective fragmentectomy. Clin Orthop Relat Res 347:150–167
Ruetten S, Komp M, Merk H, Godolias G (2009) Surgical treatment for lumbar lateral recess stenosis with the full-endoscopic interlaminar approach versus conventional microsurgical technique: a prospective, randomized, controlled study. J Neurosurg Spine 5:476–485
Yeung AT, Tsou PM (2002) Posterolateral endoscopic excision for lumbar disc herniation: surgical technique, outcome and complications in 307 consecutive cases. Spine (Phila Pa 1976) 7:722–731
Ruetten S, Komp M, Merk H, Godolias G (2007) A new full-endoscopic technique for cervical posterior foraminotomy in the treatment of lateral disc herniations using 6.9-mm endoscopes: prospective 2-year results of 87 patients. Minim Invasive Neurosurg 4:219–226
Ruetten S, Komp M, Merk H, Godolias G (2008) Full-endoscopic interlaminar and transforaminal lumbar discectomy versus conventional microsurgical technique: a prospective, randomized, controlled study. Spine (Phila Pa 1976) 9:931–939
Ruetten S, Komp M, Merk H, Godolias G (2008) Full-endoscopic cervical posterior foraminotomy for the operation of lateral disc herniations using 5.9-mm endoscopes: a prospective, randomized, controlled study. Spine (Phila Pa 1976) 9:940–948
Ruetten S, Komp M, Merk H, Godolias G (2009) Full-endoscopic anterior decompression versus conventional anterior decompression and fusion in cervical disc herniations. Int Orthop 6:1677–1682
Ruetten S, Komp M, Merk H, Godolias G (2009) Recurrent lumbar disc herniation after conventional discectomy: a prospective, randomized study comparing full-endoscopic interlaminar and transforaminal versus microsurgical revision. J Spinal Disord Tech 2:122–129
Wang B, Lü G, Patel AA, Ren P, Cheng I (2011) An evaluation of the learning curve for a complex surgical technique: the full endoscopic interlaminar approach for lumbar disc herniations. Spine J 11:122–130
Kuonsongtum V, Paiboonsirijit S, Kesornsak W, Chaiyosboorana V, Rukskul P, Chumnanvej S, Ruetten S (2009) Result of full endoscopic uniportal lumbar discectomy: preliminary report. J Med Assoc Thai 6:776–780
Cahill KS, Dunn I, Gunnarsson T, Proctor MR (2010) Lumbar microdiscectomy in pediatric patients: a large single-institution series. J Neurosurg Spine 2:165–170
Teli M, Lovi A, Brayda-Bruno M, Zagra A, Corriero A, Giudici F, Minoia L (2010) Higher risk of dural tears and recurrent herniation with lumbar micro-endoscopic discectomy. Eur Spine J 3:443–450
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wang, B., Lü, G., Liu, W. et al. Full-endoscopic interlaminar approach for the surgical treatment of lumbar disc herniation: the causes and prophylaxis of conversion to open. Arch Orthop Trauma Surg 132, 1531–1538 (2012). https://doi.org/10.1007/s00402-012-1581-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-012-1581-9