
Abstract
Introduction
We report how changes to our total hip arthroplasty (THA) surgical practise lead to a decrease in early hip dislocation rates.
Methods
Group B consisted of 421 consecutive primary THA operations performed via a posterior approach. The operative technique included a meticulous repair of the posterior capsule, alignment of the acetabular cup with the transverse acetabular ligament (TAL) and a 36-mm-diameter femoral head. We compared the dislocation rates and cost implications of this technique to a historical control Group A consisting of 389 patients. The control group had their THA performed with no repair of the capsule, no identification of the TAL and all received a 28-mm-diameter head. Our primary outcome is the rate of early hip dislocation and we hypothesised that we can reduce the rate of early hip dislocation with this new regime.
Results
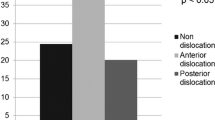
In Group B there were no early dislocations (within 6 months) and two (0.5 %) dislocations within 18 months; minimum follow-up time was 18 months with a range of (18–96 months). This compared to a 1.8 % early dislocation rate and a 2.6 % rate at 18 months in Group A; minimum follow-up time was 60 months with a range of (60–112 months). These results were statistically significant (p = 0.006).
Conclusion
We suggest that when primary hip arthroplasty is performed through a posterior approach, a low early dislocation rate can be achieved using the described methods.
Similar content being viewed by others


References
Chang RW, Pellisier JM, Hazen GB (1996) A cost-effectiveness analysis of total hip arthroplasty for osteoarthritis of the hip. JAMA 275:858–865
McCollum DE, Gray WJ (1990) Dislocation after total hip arthroplasty. Causes and prevention. Clin Orthop 261:159–170
Sanchez-Sotelo J, Haidukewych GJ, Boberg CJ (2006) Hospital cost of dislocation after primary total hip arthroplasty. J Bone Joint Surg (Am) 88:290–294
Parvizi J, Picinic E, Sharkey PF (2008) Revision total hip arthroplasty for instability: surgical techniques and principles. J Bone Joint Surg (Am) 90:1134–1142
Mahoney CR, Pellicci PM (2003) Complications in primary total hip arthroplasty: avoidance and management of dislocations. Instr Course Lect 52:247–255
Woo RY, Morrey BF (1982) Dislocations after total hip arthroplasty. J Bone Joint Surg Am 64(9):1295–1306
Biedermann R, Tonin A, Krismer M, Rachbauer F et al (2005) Reducing the risk of dislocation after total hip arthroplasty: the effect of orientation of the acetabular component. J Bone Joint Surg Br 87(6):762–769
Forsythe ME, Whitehouse SL, Dick J, Crawford RW (2007) Functional outcomes after nonrecurrent dislocation of primary total hip arthroplasty. J Arthroplasty 22:227–230
Weeden SH, Paproski WG, Bowling W (2003) The early dislocation rate in primary total hip arthroplasty following the posterior approach with posterior soft-tissue repair. J Arthroplasty 18:709–713
Horwitz BR, Rockowitz NL, Gall SR, Booth RE Jr et al (1993) A prospective randomized comparison of two surgical approaches to total hip arthroplasty. Clin Orthop Relat Res 291:154–163
Woo RY, Morrey BF (1982) Dislocations after total hip arthroplasty. J Bone Joint Surg Am 64(9):1295–1306
Dixon MC, Scott RD, Schai PA, Stamos V (2004) A simple capsulorrhaphy in a posterior approach for total hip arthroplasty. J Arthroplasty 19:373–376
Goldstein WM, Gleason TF, Kopplin M, Branson JJ (2001) Prevalence of dislocation after total hip arthroplasty through a posterolateral approach with partial capsulotomy and capsulorrhaphy. J Bone Joint Surg (Am) 83-A(Suppl 2 (Pt1)):2–7
Nishii T, Sugano N, Miki H et al (2004) Influence of component positions on dislocation: computed tomographic evaluation in a consecutive series of total hip arthroplasty. J Arthroplasty 19:162–166
Archbold HAP, Mockford B, Molloy D, McConway J, Ogonda L, Beverland D (2006) The transverse acetabular ligament: an aid to orientation of the acetabular component during primary total hip replacement. J Bone Joint Surg (Br) 88(7):883–886
Berry D, Knoch M, Schleck CD, Harmsen WS (2005) Effect of femoral head diameter and operative approach on risk of dislocation after primary total hip arthroplasty. J Bone Joint Surg (Am) 87-A:2456–2463
Kelley SS, Lachiewicz PF, Hickman JM, Paterno SM (1998) Relationship of femoral head and acetabular size to the prevalence of dislocation. Clin Orthop 355:163–170
Jameson SS, Lees D, James P, Serrano-Pedraza I, Partington PF (2011) Lower dislocation with increased femoral head size after primary total hip replacement. J Bone Joint Surg (Br) 93-B:876–880
Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR (1978) Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am 60(2):217–220
Patil S, Bergula A, Chen PC, Colwell CW Jr (2003) Polyethylene wear and acetabular component orientation. J Bone Joint Surg Am 85-A(Suppl 4):56–63
Asayama I, Akiyoshi Y, Naito M, Ezoe M (2004) Intraoperative pelvic motion in total hip arthroplasty. J Arthroplasty 19(8):992–997
No authors listed. National Joint Registry for England and Wales: sixth annual report. http://www.njrcentre.org.uk
Kotwal RS, Ganapathi M, John A, Maheson M, Jones SA (2009) Outcome of treatment for dislocation after primary total hip replacement. J Bone Joint Surg (Br) 91-B:321–326
Schuh A, Mittelmeier W, Zeiler G, Behrend D, Kircher J, Bader R (2006) Severe damage of the femoral head after dislocation and difficult reduction maneuvers after total hip arthroplasty. Arch Orthop Trauma Surg 126(2):134–137 (Epub 2006 Jan 10)
Hogarty KY, Kromrey JD (2003) RETR_PWR: an SAS macro for retrospective statistical power analysis. Behav Res Methods Instrum Comput 35:585–589
Ottenbacher KJ, Maas F (1999) How to detect effects: statistical power and evidence-based practice in occupational therapy research. Am J Occup Ther 53:181–188
Conflict of interest
No author has or will receive benefits for personal or professional use from a commercial party related directly or indirectly to the subject of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ho, K.W.K., Whitwell, G.S. & Young, S.K. Reducing the rate of early primary hip dislocation by combining a change in surgical technique and an increase in femoral head diameter to 36 mm. Arch Orthop Trauma Surg 132, 1031–1036 (2012). https://doi.org/10.1007/s00402-012-1508-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-012-1508-5