
Abstract
Purpose
This study aimed to identify and characterize patterns of fluid intake in children and adolescents from six countries: Argentina, Brazil, China, Indonesia, Mexico and Uruguay.
Methods
Data on fluid intake volume and type amongst children (4–9 years; N = 1400) and adolescents (10–17 years; N = 1781) were collected using the validated 7-day fluid-specific record (Liq.In7 record). To identify relatively distinct clusters of subjects based on eight fluid types (water, milk and its derivatives, hot beverages, sugar-sweetened beverages (SSB), 100% fruit juices, artificial/non-nutritive sweetened beverages, alcoholic beverages, other beverages), a cluster analysis (partitioning around k-medoids algorithm) was used. Clusters were then characterized according to their socio-demographics and lifestyle indicators.
Results
The six interpretable clusters identified were: low drinkers–SSB (n 523), low drinkers–water and milk (n 615), medium mixed drinkers (n 914), high drinkers–SSB (n 513), high drinkers–water (n 352) and very high drinkers–water (n 264). Country of residence was the dominant characteristic, followed by socioeconomic level, in all six patterns.
Conclusions
This analysis showed that consumption of water and SSB were the primary drivers of the clusters. In addition to country, socio-demographic and lifestyle factors played a role in determining the characteristics of each cluster. This information highlights the need to target interventions in particular populations aimed at changing fluid intake behavior and improving health in children and adolescents.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Low fluid intake, or its biomarkers, has been associated with an increased risk of developing cardiometabolic diseases [1, 2], chronic kidney disease [3] and recurrent kidney stones [4]. Adequate hydration has been shown to improve cognition in children [5] and adults [6], improve mood [7, 8] and attenuate biological risk factors for the above-mentioned conditions. In addition, consuming sugar-sweetened beverages (SSB) has been linked with an increased future risk of obesity [9], and cardiometabolic diseases. Each daily serving increase in SSB has been linked to a 21% increased risk of type 2 diabetes [10], 7% increased risk of hypertension [11] and 7–18% increased risk of stroke, heart failure and coronary heart disease [12].
Total fluid intake has been reported for many countries [13,14,15,16,17,18,19,20] together with data on the type of fluid consumed [21,22,23,24,25]. Many studies have shown that a high proportion of children and adolescents do not drink enough to meet water intake recommendations [13, 15, 16, 23]. This is especially important in young children who, due to their relatively high body water content and underdeveloped regulatory systems, are vulnerable to the effects of not drinking enough [26]. It is apparent from these, and many other studies, that while an individual may be drinking sufficient in terms of volume to meet, or exceed current recommendations on fluid intake, there may be a wide variety of combinations of fluid type within that total volume. Considering only one or two variables at a time limits the interpretation of data, and as a consequence, their usefulness [27]. Increasingly, dietary patterns are being studied to investigate these interactions [28]. Therefore, it is now pertinent to look at patterns of fluid consumption as opposed to studies that consider only volume or individual fluid type.
Different methods of analyzing dietary patterns can be used in diverse populations, including principal component analysis, cluster analyses and more recently, reduced rank regression [29]. Fluid intake has been evaluated using multiple regression analysis [19], principal component analysis [30] and a dynamic panel model [31]. Another multivariate technique that can be applied to fluid intake is cluster analysis. The main advantage of cluster analysis is that it creates groups of individuals that are as homogeneous as possible, minimizing the variance within each group and maximizing the variance between groups. This allows the identification of fluid intake patterns, called ‘clusters’, common to a group of people that are different from each of the other patterns. Such clusters can then be evaluated through classical regression methods, interpreted and validated from a fluid intake point of view. Cluster analysis has been used extensively to evaluate dietary patterns [32], and is now being applied to fluid intake patterns in adults [17, 33, 34] and children [35,36,37,38,39], although its use is still limited.
However, to the best of our knowledge cluster analysis of fluid intake patterns in children and adolescents has only been performed in single-country population groups. A global analysis of FI patterns has not been possible to date due to variations in the methodology used to collect data; therefore, the importance of the country of residence per se has not been investigated using cluster analysis. With the availability of a validated 7-day fluid record [40] and a harmonized methodology across various countries [41,42,43] it is now possible to study global fluid intake patterns taking into consideration this variable. Therefore, the primary aim of this study was to identify different patterns of fluid intake in children and adolescents in six countries. The secondary aim was to characterize these patterns in terms of socio-demographics and lifestyle indicators.
Materials and methods
Survey and survey sample
This pooled secondary analysis was performed on the individual data of 3214 participants aged 4–17.9 years from six cross-sectional surveys. The primary objective of all surveys was to assess the intake of drinking water and different types of beverages. The surveys included in the pooled analysis were conducted in Latin America (Mexico, Brazil, Argentina, Uruguay), and Asia (China, Indonesia) in 2016. The recruitment of participants and further details of the populations included in this analysis have been described previously [41,42,43].
Participants and parents were selected from a database of individuals volunteering for population surveys or via a systematic door-to-door approach with an invitation for their child to participate. All participants, including parents and children, willing to join in the survey received detailed information about the survey objectives, what was expected from them, as well as a disclosure of the survey’s provisions to preserve confidentiality, risks and benefits, and a clear explanation about their option to participate voluntarily or not in the survey. After offering a detailed description of the survey, parents were asked for oral approval for their child to participate. No monetary incentive was offered for taking part in the survey. All data were recorded anonymously. Therefore, participants cannot be identified directly, or through identifiers linked to the participants. The survey protocol was reviewed and approved by the University of Arkansas Review Board (ref. 14-12-376).
Fluid assessment
Participants were provided with the Liq.In7 record, a 7-day fluid-specific record validated for accuracy and reliability [40]. The Liq.In7 record was presented in the official country language. In all countries, except China, a paper version of the record was delivered and explained to the participants during an interview at home. After a period of 7 days, the record was collected by the researcher and checked for completion with the participant. In China, participants completed an electronic version of the Liq.In7 record via a smart phone. Participants were instructed to report all drinking events at any moment of the day with details such as the fluid type, size of the container from which the fluid was drunk and the actual volume consumed. Food consumption was not recorded. To assist participants in estimating the precise volume of fluid consumed, a photographic booklet of standard fluid containers supported the records. For children younger than 12 years, the primary caregiver was responsible for completing the record.
Anthropometric and lifestyle variables
The anthropometric and lifestyle data were collected via a questionnaire during a face-to-face visit at home, except in China where these data were collected via a web-based questionnaire. In all countries, except for Indonesia, height (m) and weight (kg) were self-reported by participants or caregivers depending on the participant’s age. In Indonesia, weight was measured by the survey researchers. The body mass index (BMI) was calculated (kg/m2); BMI classification was based on sex- and age-specific cut-off values for individuals aged ≤ 18 years [44].
To determine the socioeconomic status (SES) of each participant, country-adapted classifications were applied. In Mexico, Argentina and Uruguay, the Asociación Mexicana de Agencias de Investigación de Mercado y Opinión Pública (AMAI) system was used and in Brazil the ABEP classification [45, 46]. Both systems use a combination of the following criteria to determine the SES of a household; work status, occupation, education, medical coverage, number of domestic servants, number of bathrooms, household equipment, possession of an international credit card and/or access to public utility services. In Indonesia, SES was determined based on the combined score of household expenditure, electricity usage, household cooking equipment and the kind of source of drinking water (e.g., tap water, well water, spring water) for use in the household. In China, SES was determined based on the household income of the participant. An income of RMB ≤ 5999 was classified as SES DE, an income between RMB 6000 and 11,999 as SES C and an income ≥ RMB 12,000 as level AB. For this analysis, SES classes were harmonized as detailed in Table S1 of the online resources.
The number of hours per day the participant spent watching TV or any content on a screen (≥ 2 or < 2 h/day) was considered as a proxy for sedentary behavior. The frequency of any exercise or sports, independent of the intensity, was recorded. To evaluate the availability of fluids at school, the following question was included in the questionnaire: “At school, is there a drinking fountain of water, a vending machine for beverages and/or a snack shop inside school available?” Moreover, the use of a lunchbox was assessed with the question “How often do you prepare a lunchbox for your child to go to school?” All variables and their modalities are listed in the Online Resource Table S2.
Classification and analysis of fluid types
The fluids recorded were classified into the following eight categories: water (tap and bottled water); milk and milk derivatives; hot beverages (coffee, tea and other hot beverages); 100% fruit juices; SSB (carbonated soft drinks (CSD), juice-based drinks, functional beverages, e.g., energy and sports drinks, ready to drink tea and coffee and flavored water); artificial/non-nutritive sweetened beverages (A/NSB) (diet/zero/light soft drinks); alcoholic beverages and other beverages. Full details are given in Online Resource Table S3. Volumes of all categories were summed to give TFI.
Statistical analysis
Participants who did not complete the full 7-day fluid record, and/or participants reporting a mean total daily fluid intake below 0.4 L/day, physiologically the minimum daily urine production [47], or higher than 6 L/day, were excluded from the analysis (Fig. 1). Only participants who had all socio-demographic and lifestyle indicators were included in the characterization of the cluster. Consequently, 628 subjects were excluded from the characterization (Fig. 1). The partitioning around medoids (PAM) method of R package ‘Cluster’ [48] was applied to the mean intake of the eight fluid types. PAM method is an unsupervised clustering method which needs an a priori number of clusters. To select the optimal number of clusters, a two-step approach was applied: the first step was to test several clusterings with different number of clusters from 2 to 50. For each clustering, the average silhouette coefficient, a statistical indicator to evaluate the robustness of the clustering, was computed (Online resources Fig S1). Only those clusterings with an average silhouette coefficient greater than 0.25 and a sample size balanced enough between clusters were considered statistically robust enough to go on to the second step, being the interpretability check. Remaining clusterings were then evaluated from a fluid intake point of view and the most interpretable one was chosen as the optimal clustering. Interpretability was evaluated by the predominant fluid intake within a cluster and the difference between clusters.

Flowchart showing sample selection for clustering and characterization
For fluid intake comparisons between clusters, a one-way ANOVA was used with clusters as factors. To correct for multiple testing over the different fluid types, Benjamini–Hochberg correction was used. When significant, Tukey post hoc tests were used to determine which clusters were different. ANOVA and post hoc tests were performed using JMP® v12 software (SAS Institute Inc., Cary, NC, USA). For characterization of clusters with socio-demographics and lifestyles indicators, the “catdes” function of FactoMineR [49], an R package, was used. For stringency purposes, clusters’ characteristics were selected as being significant at a 0.1% level and ranked by their v test from the highest to the lowest. The v tests can be interpreted in the same way as Z scores: the higher the v test, the stronger the characteristic. Positive v test means an over-representation and negative an under-representation. Chi-square tests were used to evaluate differences between clusters for categorical variables (Online Resource Table S2).
Results
Identification of drinking patterns
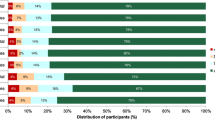
Fifteen clusters showed a silhouette coefficient greater than 0.25 (Online resources Figure S1). Different numbers of clusters were explored before selecting an analysis based on six fluid patterns (clusters), as this was the most interpretable based on fluid intake amount/composition. The daily total fluid intake (TFI) of each cluster is shown in Table 1 and Fig. 2. Predominant fluid volume and fluid type for each cluster are highlighted in bold in Table 1. The six fluid patterns were: low drinkers–SSB (n 523; 16%), low drinkers–water and milk (n 615; 19%), medium mixed drinkers (n 914; 29%), high drinkers–SSB (n 513; 16%), high drinkers–water (n 352; 11%) and very high drinkers–water (n 264; 8%). The largest cluster was medium mixed drinkers, which represented 29% of the total sample.

Mean daily intake of different fluid types (mL/day) of each cluster among children and adolescents. SSB sugar-sweetened beverages, A/NSB artificial/non-nutritive-sweetened beverages
Comparisons between drinking pattern clusters
Mean water intake was significantly different between clusters (Table 1). The low drinkers–water and milk cluster had a significantly lower water intake compared with the medium mixed drinkers, high drinkers–water and the very high drinkers–water, and a higher water intake compared with the cluster low drinkers–SSB. No significant difference in water intake was observed between the low drinkers–water and milk and high drinkers–SSB clusters. The low drinkers–water and milk cluster consumed significantly more milk than any of the other clusters and had a significantly lower intake of hot beverages compared with all the other clusters. No significant difference in hot beverage intake was observed between the high drinkers–SSB, low drinkers–SSB, high drinkers–water and very high drinkers–water clusters and between the medium mixed drinkers, high and very high drinkers–water clusters. The high drinkers–SSB cluster had a significantly higher intake of SSB compared with all the other clusters. Low drinkers–SSB and high drinkers–water clusters had significantly higher SSB intakes compared with the medium mixed drinkers, the low drinkers–water and milk and the very high drinkers–water.
Characterization of the fluid intake patterns
The characteristics of the six FI patterns are shown in Table 2(a–f). Country of residence was the dominant characteristic in all six patterns. The low drinkers–SSB cluster (Table 2(a)) had an over-representation of Brazilians (33%), Mexicans (27%) and to a lesser extent Argentinians (22%). Indonesians were under-represented in this cluster (2%).
The most significant characteristic associated with low drinkers–water and milk (Table 2(b)) was again the country of residence, with 51% of Chinese participants represented in this cluster. Other characteristics over-represented in this cluster included having sedentary behavior approximated by a screen time of more than 2 h/day, being of higher SES class (AB), frequently having a lunch box (daily or nearly daily), being in the younger age group (4–9 years) and having a fluid source available at school. The characteristics that were under-represented in this cluster were residing in Argentina (9%) or Indonesia (3%). Adolescents (ages 10–17 years) and the children who did not have a lunchbox prepared daily by their parents were also under-represented in this cluster.
The country of residence was the only significant characteristic of the medium mixed drinkers cluster (Table 2(c)). Indonesian participants were over-represented in this cluster, with 38%. In this cluster, Argentinian and Mexican were both under-represented.
Residents in Argentina, Uruguay and Mexico were over-represented in the high drinkers–SSB cluster (Table 2(d)) with 44, 32 and 22% of these countries’ participants, respectively. The other characteristics over-represented in this cluster were children and adolescents from the lowest socioeconomic class (DE), having a sedentary behavior ≥ 2 h/day, never or rarely taking a lunchbox to school nor having available fluids at school and being overweight. Chinese and Indonesian residents were significantly under-represented in this cluster with only 4% from China and 1% from Indonesia.
The defining characteristics of the high drinkers–water cluster (Table 2(e)) were country and physical activity. Twenty-nine percent of Indonesians were in this cluster compared with 4% from Brazil and 3% each from China, Uruguay and Argentina. Participants who reported being physically active once a week to twice monthly were over-represented in this cluster as was sedentary behavior of 2 or more hours/day.
The very high drinkers–water FI pattern cluster (Table 2(f)) had an over-representation of Indonesians, the other five countries being under-represented. The other characteristics that were over-represented in this cluster were being in SES C, being underweight and having a physical activity level of once a week to twice a month.
Discussion
Cluster analysis enables the identification of behaviors and associated characteristics, which may help target the specific populations that require intervention to change behavior. Unlike other cluster analyses, that have looked at fluid intake types in the context of energy content [35, 38], or diet quality [36], the emphasis of this analysis was drinking behavior. A total of eight fluid types were used in this cluster analysis to identify fluid intake patterns in children and adolescents across six countries. The first observation was that the FI patterns in this analysis were driven by SSB and water, and to a lesser extent milk and its derivatives. The second most striking observation was that the most significant characteristic across the FI patterns was country of residence. The Latin American countries were more represented in the low drinkers–SSB or the high drinkers–SSB FI patterns. These results are consistent with reports based on volumes of fluid types consumed [21, 42]. High intakes of SSB in Latin American countries have already raised concerns given the associations with dental caries [50], obesity and overweight [51] and associated metabolic conditions among children and adolescent [52]. In addition to high SSB intake, residence in Brazil, Mexico and Argentina was associated with low total fluid intake (low drinkers–SSB). The mean total fluid intake for this cluster was 1 L/day, which compares unfavorably with recommendations on the adequate intake of water from fluids [53]. Children and adolescents in these countries may be at risk of suboptimal hydration [54], which is associated with impaired cognition and low mood [55] and physical performance [56]. Uruguayan children and adolescents had high TFI and were over-represented in the high drinkers–SSB pattern. Therefore, interventions may be most effective if targeted at replacing energy-containing drink with water while maintaining the TFI. This analysis suggests that interventions in these countries should be targeted at increasing drinking water consumption while reducing sugar fluid intake. Some countries, including Mexico [57], are adopting this approach by introducing taxes to increase the price of sugar drinks; it is possible that this will particularly influence those in lower SELs [58].
Chinese residents were predominantly in the low drinkers–water and milk FI cluster (51%); a pattern in which the younger children (4–9 years) were over-represented; as were taking a lunch box to school and having fluid available at school. This pattern appears to reflect the policies implemented in China whereby a school lunch that includes a serving of 250 mL of milk is provided to first and middle-school children [59, 60]. Indonesians were over-represented in both the high drinkers– and very high drinkers–water patterns; these FI patterns have TFIs > 2.5 L/day as shown in a previous analysis [41]. From the present analysis, it would appear that in terms of fluid volume and type, there is little of concern that requires intervention in these latter two clusters. This could be due to all proactive actions undertaken in Indonesia to increase the access to safe water [61] and to encourage water consumption [62]. However, with increasing levels of obesity [63] and type 2 diabetes [64] in Indonesia there are concerns about increasing SSB consumption [65]. Public health policies and interventions are needed to halt and hopefully reverse this trend [66].
Fluid pattern analyses in children and adolescents have been conducted in the USA [30] and Canada [35]. Bougatsas et al. identified six clusters [30] including one which was similar to the low drinkers–water and milk cluster. Other comparisons between the two analyses are difficult due to the differences in fluid type classification. The analysis by Danyliw and colleagues [35] identified five clusters including milk and high-fat milk; however, water was excluded from the analysis as fluids were categorized on the basis of their energy and nutrient content. Other analyses have concentrated entirely on energy content rather than volume of fluid types. This is the first study to include data from more than one country; therefore, direct comparisons to other analyses are difficult and reasons for any similarities or differences are beyond the remit of the present analysis. However, while societal and cultural influences on food patterns are well recognized [67], identification of the factors that influence drinking patterns requires further research.
Socioeconomic level was a significant characteristic in three of the FI clusters. The low drinkers–milk and water cluster was more represented by SES AB, high drinkers–SSB were associated with SES DE and very high drinkers–water were associated with SES C. Disparities in SES and hydration [68], water [69] and type of fluids consumed [70] have been reported although evidence from cluster analysis is limited and complicated by the lack of consistent definitions of SEL. Danyliw et al. [35] noted differences in intake according to household security and income, but no specific patterns were established. In a recent systematic review lower SES was associated with higher SSB consumption [71]. In the present analysis, a lower SES was also a significant characteristic of the high intake–SSB cluster. Therefore, it would seem appropriate for interventions in those countries that aim to decrease SSB consumption and replace SSB with water, target children and adolescents in the lower SELs.
Sedentary behavior and/or physical activity were significant characteristics of four of the FI pattern clusters. Participants who reported less than 2 h of sedentary behavior were over-represented in the low drinkers–water and milk cluster. Children and adolescents who reported more than 2 h of sedentary behavior were over-represented in the high drinkers with SSB cluster; those who reported being physically active once a week to twice a month were under-represented. A recent cluster analysis of data from the ELANA and HELENA studies in children and adolescents reported clusters characterized by sedentary behavior and SSB consumption [72]. This is not surprising given the established links between sedentary behavior and less healthy dietary intake including SSB consumption [71, 73, 74]. Those who reported sedentary behavior greater than 2 h a week and/or being physically active once a week to twice a month were over-represented in the very high drinkers–water cluster. While this may appear contradictory, this phenomenon has been reported before and is probably due to those who report being sedentary for two or more hours per day compensating by being physically active at other times of the day [72]. Clearly, the prevention and treatment of overweight and obesity in children and adolescents requires a multifaceted approach, which focuses on changing dietary habits, including reducing SSB consumption, and reducing sedentary behavior and or increasing physical activity.
The current study has several strengths including the use of a harmonized sampling and data collection methodology across the countries and of a validated assessment method for total fluid intake [40], reflecting the day-to-day behavior of the participants over a 7-day period. The sample size and the use of data from participants in six countries undoubtedly strengthened the analysis. Objective statistical criteria such as using the silhouette coefficient to identify the number of clusters combined with the subsequent use of subjective criteria rendered the selected clusters interpretable. However, it is important to recognize the limitations of this study. Missing data for some of the variables resulted in a slightly reduced sample size; however, this is inevitable in large cross-sectional studies such as the Liq.In7 survey. The use of biomarkers for hydration status or health outcome measures would have strengthened the findings and possible implications of the analysis. Parents or primary carers recorded fluid intake and responded to questions about lifestyle and socio-demographics for younger participants, while this may have increased precision they may have been biased towards demonstrated healthy characteristics. In addition, adolescents were not asked if their parents provided a lunchbox for school nor about water availability in schools. While the questions on sedentary behavior and physical activity provide vital and interesting information, it would have been better to have used a validated physical activity questionnaire such as the International Physical Activity Questionnaire (IPAQ). To ensure a reliable and sensitive approximation of socioeconomic status, country-specific methods were used as a harmonized classification system is not currently available.
This analysis is the first to investigate fluid intake patterns across countries and has shown that country of residence is an important determinant of cluster membership. Therefore, it would be interesting to repeat the analysis within each country and extend the survey to other countries and regions of the world. Given the interest in establishing guidance and recommendations across regions, e.g., Latin American countries, or continents, e.g., Europe, once more data are available it would be interesting to repeat the analysis again within these regions. Cluster analysis of fluid intake patterns could be a useful tool for monitoring interventions aimed at increasing water intake while reducing SSB consumption by repeating the analysis over a period of time.
Conclusions
This analysis identified six clusters with differing fluid intake patterns, which varied in terms of total fluid intake. The consumption of water and SSB was the primary drivers of the clusters. Country of residence proved to be an important variable, with some countries being over- or under-represented in the clusters. In addition, socio-demographic and lifestyle factors played a role in determining the characteristics of each cluster. Together this information highlights the need to target interventions in particular populations aimed at changing fluid intake behavior and improving health, e.g., increasing water intake and reducing SSB consumption in Mexico. This analysis emphasizes the need for more local surveys to provide valuable data for the development, implementation and evaluation of policies and programs aimed at changing fluid intake behavior.
References
Roussel R, Fezeu L, Bouby N, Balkau B, Lantieri O, Alhenc-Gelas F, Marre M, Bankir L (2011) Low water intake and risk for new-onset hyperglycemia. Diabetes Care 34(12):2551–2554. https://doi.org/10.2337/dc11-0652
Guelinckx I, Vecchio M, Perrier ET, Lemetais G (2016) Fluid intake and vasopressin: connecting the dots. Ann Nutr Metab 68(suppl 2):6–11. https://doi.org/10.1159/000446198
Strippoli GF, Craig JC, Rochtchina E, Flood VM, Wang JJ, Mitchell P (2011) Fluid and nutrient intake and risk of chronic kidney disease. Nephrology (Carlton) 16(3):326–334. https://doi.org/10.1111/j.1440-1797.2010.01415.x
Lotan Y, Daudon M, Bruyere F, Talaska G, Strippoli G, Johnson RJ, Tack I (2013) Impact of fluid intake in the prevention of urinary system diseases: a brief review. Curr Opin Nephrol Hypertens 22(Suppl 1):S1–S10. https://doi.org/10.1097/MNH.0b013e328360a268
Edmonds CJ, Burford D (2009) Should children drink more water? The effects of drinking water on cognition in children. Appetite 52(3):776–779. https://doi.org/10.1016/j.appet.2009.02.010
Ganio MS, Armstrong LE, Casa DJ, McDermott BP, Lee EC, Yamamoto LM, Marzano S, Lopez RM, Jimenez L, Le BL, Chevillotte E, Lieberman HR (2011) Mild dehydration impairs cognitive performance and mood of men. Br J Nutr 106(10):1535–1543. https://doi.org/10.1017/S0007114511002005
Pross N, Demazieres A, Girard N, Barnouin R, Metzger D, Klein A, Perrier E, Guelinckx I (2014) Effects of changes in water intake on mood of high and low drinkers. PLoS One 9(4):e94754. https://doi.org/10.1371/journal.pone.0094754
Pross N, Demazieres A, Girard N, Barnouin R, Santoro F, Chevillotte E, Klein A, Le BL (2013) Influence of progressive fluid restriction on mood and physiological markers of dehydration in women. Br J Nutr 109(2):313–321
Malik VS, Pan A, Willett WC, Hu FB (2013) Sugar-sweetened beverages and weight gain in children and adults: a systematic review and meta-analysis. Am J Clin Nutr 98(4):1084–1102. https://doi.org/10.3945/ajcn.113.058362
Schwingshackl L, Hoffmann G, Lampousi AM, Knuppel S, Iqbal K, Schwedhelm C, Bechthold A, Schlesinger S, Boeing H (2017) Food groups and risk of type 2 diabetes mellitus: a systematic review and meta-analysis of prospective studies. Eur J Epidemiol 32(5):363–375. https://doi.org/10.1007/s10654-017-0246-y
Schwingshackl L, Schwedhelm C, Hoffmann G, Knuppel S, Iqbal K, Andriolo V, Bechthold A, Schlesinger S, Boeing H (2017) Food groups and risk of hypertension: a systematic review and dose-response meta-analysis of prospective studies. Adv Nutr 8(6):793–803. https://doi.org/10.3945/an.117.017178
Bechthold A, Boeing H, Schwedhelm C, Hoffmann G, Knuppel S, Iqbal K, De Henauw S, Michels N, Devleesschauwer B, Schlesinger S, Schwingshackl L (2017) Food groups and risk of coronary heart disease, stroke and heart failure: a systematic review and dose-response meta-analysis of prospective studies. Crit Rev Food Sci Nutr. https://doi.org/10.1080/10408398.2017.1392288
Iglesia I, Guelinckx I, De Miguel-Etayo PM, Gonzalez-Gil EM, Salas-Salvado J, Kavouras SA, Gandy J, Martinez H, Bardosono S, Abdollahi M, Nasseri E, Jarosz A, Ma G, Carmuega E, Thiebaut I, Moreno LA (2015) Total fluid intake of children and adolescents: cross-sectional surveys in 13 countries worldwide. Eur J Nutr 54(Suppl 2):57–67. https://doi.org/10.1007/s00394-015-0946-6
Ferreira-Pego C, Nissensohn M, Kavouras SA, Babio N, Serra-Majem L, Martin Aguila A, Mauromoustakos A, Alvarez Perez J, Salas-Salvado J (2016) Beverage intake assessment questionnaire: relative validity and repeatability in a Spanish population with metabolic syndrome from the PREDIMED-PLUS study. Nutrients 8(8):475. https://doi.org/10.3390/nu8080475
Vieux F, Maillot M, Constant F, Drewnowski A (2016) Water and beverage consumption among children aged 4–13 years in France: analyses of INCA 2 (Etude Individuelle Nationale des Consommations Alimentaires 2006–2007) data. Public Health Nutr 19(13):2305–2314. https://doi.org/10.1017/s1368980015003614
Sui Z, Zheng M, Zhang M, Rangan A (2016) Water and beverage consumption: analysis of the Australian 2011–2012 national nutrition and physical activity survey. Nutrients 8(11):678. https://doi.org/10.3390/nu8110678
Popkin BM, Barclay DV, Nielsen SJ (2005) Water and food consumption patterns of U.S. adults from 1999 to 2001. Obes Res 13(12):2146–2152. https://doi.org/10.1038/oby.2005.266
Tani Y, Asakura K, Sasaki S, Hirota N, Notsu A, Todoriki H, Miura A, Fukui M, Date C (2015) The influence of season and air temperature on water intake by food groups in a sample of free-living Japanese adults. Eur J Clin Nutr 69(8):907–913. https://doi.org/10.1038/ejcn.2014.290
Lee KW, Shin D, Song WO (2016) Total water intake from beverages and foods is associated with energy intake and eating behaviors in Korean adults. Nutrients 8(10):617. https://doi.org/10.3390/nu8100617
Ma G, Zhang Q, Liu A, Zuo J, Zhang W, Zou S, Li X, Lu L, Pan H, Hu X (2012) Fluid intake of adults in four Chinese cities. Nutr Rev 70(Suppl 2):S105–S110. https://doi.org/10.1111/j.1753-4887.2012.00520.x
Guelinckx I, Iglesia I, Bottin JH, De Miguel-Etayo P, Gonzalez-Gil EM, Salas-Salvado J, Kavouras SA, Gandy J, Martinez H, Bardosono S, Abdollahi M, Nasseri E, Jarosz A, Ma G, Carmuega E, Thiebaut I, Moreno LA (2015) Intake of water and beverages of children and adolescents in 13 countries. Eur J Nutr 54(S2):69–79. https://doi.org/10.1007/s00394-015-0955-5
Guelinckx I, Ferreira-Pego C, Moreno LA, Kavouras SA, Gandy J, Martinez H, Bardosono S, Abdollahi M, Nasseri E, Jarosz A, Ma G, Carmuega E, Babio N, Salas-Salvado J (2015) Intake of water and different beverages in adults across 13 countries. Eur J Nutr 54(S2):S45–S55
Vieux F, Maillot M, Constant F, Drewnowski A (2017) Water and beverage consumption patterns among 4 to 13-year-old children in the United Kingdom. BMC Public Health 17(1):479. https://doi.org/10.1186/s12889-017-4400-y
Nissensohn M, Castro-Quezada I, Serra-Majem L (2013) Beverage and water intake of healthy adults in some European countries. Int J Food Sci Nutr 64(7):801–805. https://doi.org/10.3109/09637486.2013.801406
Paulsen MM, Myhre JB, Andersen LF (2016) Beverage consumption patterns among Norwegian adults. Nutrients 8(9):561. https://doi.org/10.3390/nu8090561
Manz F (2007) Hydration in children. J Am Coll Nutr 26(S5):562–569. https://doi.org/10.1080/07315724.2007.10719659
Miller JM, Guo Y, Rodseth SB (2011) Cluster analysis of intake, output, and voiding habits collected from diary data. Nurs Res 60(2):115–123. https://doi.org/10.1097/NNR.0b013e3182097813
Leech RM, Worsley A, Timperio A, McNaughton SA (2015) Understanding meal patterns: definitions, methodology and impact on nutrient intake and diet quality. Nutr Res Rev 28(1):1–21. https://doi.org/10.1017/S0954422414000262
Tucker KL (2010) Dietary patterns, approaches, and multicultural perspective. Appl Physiol Nutr Metab 35(2):211–218. https://doi.org/10.1139/H10-010
Bougatsas D, Arnaoutis G, Panagiotakos DB, Seal AD, Johnson EC, Bottin JH, Tsipouridi S, Kavouras SA (2017) Fluid consumption pattern and hydration among 8–14 years-old children. Eur J Clin Nutr 72(3):420–427. https://doi.org/10.1038/s41430-017-0012-y
Piernas C, Ng SW, Mendez MA, Gordon-Larsen P, Popkin BM (2015) A dynamic panel model of the associations of sweetened beverage purchases with dietary quality and food-purchasing patterns. Am J Epidemiol 181(9):661–671. https://doi.org/10.1093/aje/kwu317
Devlin UM, McNulty BA, Nugent AP, Gibney MJ (2012) The use of cluster analysis to derive dietary patterns: methodological considerations, reproducibility, validity and the effect of energy mis-reporting. Proc Nutr Soc 71(4):599–609. https://doi.org/10.1017/S0029665112000729
Duffey KJ, Popkin BM (2006) Adults with healthier dietary patterns have healthier beverage patterns. J Nutr 136(11):2901–2907. https://doi.org/10.1093/jn/136.11.2901
Nikpartow N, Danyliw AD, Whiting SJ, Lim HJ, Vatanparast H (2012) Beverage consumption patterns of Canadian adults aged 19 to 65 years. Public Health Nutr 15(12):2175–2184. https://doi.org/10.1017/S1368980012003898
Danyliw AD, Vatanparast H, Nikpartow N, Whiting SJ (2011) Beverage intake patterns of Canadian children and adolescents. Public Health Nutr 14(11):1961–1969. https://doi.org/10.1017/S1368980011001091
LaRowe TL, Moeller SM, Adams AK (2007) Beverage patterns, diet quality, and body mass index of US preschool and school-aged children. J Am Diet Assoc 107(7):1124–1133. https://doi.org/10.1016/j.jada.2007.04.013
Lopez-Olmedo N, Jimenez-Aguilar A, Morales-Ruan MDC, Hernandez-Avila M, Shamah-Levy T, Rivera-Dommarco JA (2017) Consumption of foods and beverages in elementary schools: results of the implementation of the general guidelines for foods and beverages sales in elementary schools in Mexico, stages II and III. Eval Program Plann 66:1–6. https://doi.org/10.1016/j.evalprogplan.2017.08.009
Schroder H, Mendez MA, Ribas L, Funtikova AN, Gomez SF, Fito M, Aranceta J, Serra-Majem L (2014) Caloric beverage drinking patterns are differentially associated with diet quality and adiposity among Spanish girls and boys. Eur J Pediatr 173(9):1169–1177. https://doi.org/10.1007/s00431-014-2302-x
Marshall TA, Van Buren JM, Warren JJ, Cavanaugh JE, Levy SM (2017) Beverage consumption patterns at age 13 to 17 years are associated with weight, height, and body mass index at age 17 years. J Acad Nutr Diet 117(5):698–706. https://doi.org/10.1016/j.jand.2017.01.010
Johnson EC, Peronnet F, Jansen LT, Capitan-Jimenez C, Adams JD, Guelinckx I, Jimenez L, Mauromoustakos A, Kavouras SA (2017) Validation testing demonstrates efficacy of a 7-day fluid record to estimate daily water intake in adult men and women when compared with total body water turnover measurement. J Nutr 147(10):2001–2007. https://doi.org/10.3945/jn.117.253377
Purwita MC, Gandy J, Moreno LA, Kavouras SA, Martinez H, Salas-Salvadó J, Guelinckx I (2018) Fluid intake in Indonesia: results of the 2016 Liq.In7 National Cross-Sectional Survey. Eur J Nutr Suppl (submitted for publication)
Gandy J, Martinez H, Carmuega E, Arredondo JL, Pimmental C, Moreno LA, Kavouras SA, Salas-Salvadó J, Guelinckx I (2018) Fluid intake of Latin American children and adolescents: results of four 2016 Liq.In7 national cross-sectional surveys. Eur J Nutr Suppl (submitted for publication)
Zhang NMC, Guelinckx I, Moreno LA, Kavouras SA, Gandy J, Martinez H, Salas-Salvadó J, Ma G (2018) Fluid intake in China: results of the 2016 Liq.In7 national cross-sectional surveys. Eur J Nutr Suppl (submitted for publication)
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH (2000) Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 320(7244):1240–1243. https://doi.org/10.1136/bmj.320.7244.1240
Asociación Mexicana de Inteligencia de Mercado y Opinión (AMAI) (2016). Niveles Socio Económicos (NSE). http://nse.amai.org/. Accessed 22 Feb 2018
Associacao Brasileira de Empresas de Pesquisa (2015) Brazilian Criteria and social class distribution update for 2016. http://www.abep.org/criterio-brasil. Accessed 22 Feb 2018
Klahr S, Miller SB (1998) Acute oliguria. N Engl J Med 338(10):671–675. https://doi.org/10.1056/NEJM199803053381007
Maechler M, Rousseeuw P, Struyf A, Hubert M, Hornik K (2015) Cluster: cluster analysis basics and extensions. R Package
Husson F, Josse J, Le S, Mazet J (2014) FactoMineR: multivariate exploratory data analysis and data mining with R. http://CRAN.R-project.org/package=FactoMineR. http://factominer.free.fr/factomethods/categories-description.html. Accessed 22 Feb 2018
Moynihan PJ, Kelly SA (2014) Effect on caries of restricting sugars intake: systematic review to inform WHO guidelines. J Dent Res 93(1):8–18. https://doi.org/10.1177/0022034513508954
Katzmarzyk PT, Broyles ST, Champagne CM, Chaput JP, Fogelholm M, Hu G, Kuriyan R, Kurpad A, Lambert EV, Maia J, Matsudo V, Olds T, Onywera V, Sarmiento OL, Standage M, Tremblay MS, Tudor-Locke C, Zhao P (2016) Relationship between soft drink consumption and obesity in 9–11 years old children in a multi-national study. Nutrients 8(12):770. https://doi.org/10.3390/nu8120770
Rivera JA, Barquera S, Campirano F, Campos I, Safdie M, Tovar V (2002) Epidemiological and nutritional transition in Mexico: rapid increase of non-communicable chronic diseases and obesity. Public Health Nutr 5(1A):113–122. https://doi.org/10.1079/PHN2001282
Institute of Medicine, Food and Nutrition Board (2004) Dietary reference intakes for water, potassium, sodium, chloride and sulfate. National Academies Press, Washington DC. https://www.nap.edu/catalog/10925/dietary-reference-intakes-for-water-potassium-sodium-chloride-and-sulfate. Accessed 12 May 2018
Kavouras SA, Johnson EC, Bougatsas D, Arnaoutis G, Panagiotakos DB, Perrier E, Klein A (2015) Validation of the urine color scale in children. Eur J Nutr 55:907–915. https://doi.org/10.1007/s00394-015-0905-2
Benton D, Burgess N (2009) The effect of the consumption of water on the memory and attention of children. Appetite 53(1):143–146. https://doi.org/10.1016/j.appet.2009.05.006
Kavouras SA, Arnaoutis G, Makrillos M, Garagouni C, Nikolaou E, Chira O, Ellinikaki E, Sidossis LS (2011) Educational intervention on water intake improves hydration status and enhances exercise performance in athletic youth. Scand J Med Sci Sports 22(5):684–689. https://doi.org/10.1111/j.1600-0838.2011.01296.x
Sanchez-Romero LM, Penko J, Coxson PG, Fernandez A, Mason A, Moran AE, Avila-Burgos L, Odden M, Barquera S, Bibbins-Domingo K (2016) Projected impact of Mexico’s sugar-sweetened beverage tax policy on diabetes and cardiovascular disease: a modeling study. PLoS Med 13(11):e1002158. https://doi.org/10.1371/journal.pmed.1002158
Paraje G (2016) The effect of price and socio-economic level on the consumption of sugar-sweetened beverages (SSB): the case of Ecuador. PLoS One 11(3):e0152260. https://doi.org/10.1371/journal.pone.0152260
Wang TZQ, Pan H, Gan Q, Li L, Yang T, Xing Q, Hu X (2016) Food intake of students from nutrition improvement programme for rural compulsory education students in 2013. Chin J School Health 37(5):670–673
Dairy Association of China (2017) White paper of Chinese dairy industry: School Milk Program has benefited more than 20 million primary and middle school students. Anim Husb Xinjiang 7:62. https://doi.org/10.3969/j.issn.1003-4889.2017.07.032
WHO/UNICEF Progress on Drinking Water (2017) Sanitation and Hygiene. http://www.who.int/water_sanitation_health/publications/jmp-2017/en/ Accessed 22 Feb 2018
Kementerian Kesehatan RI (2014) Pedoman Gizi Seimbang. http://gizi.depkes.go.id/download/Pedoman%20Gizi/PGS%20Ok.pdf. Accessed 2 Feb 2018
Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C et al (2014) Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 384(9945):766–781. https://doi.org/10.1016/S0140-6736(14)60460-8
Prevalence of diabetes in the WHO South-East Asia Region (2017) http://www.who.int/diabetes/facts/world_figures/en/index5.html. Accessed 22 Feb 2018
Atmarita MPH IN, Jahari AB, Permaesih D, Chan P, Amarra MS (2017) Consumption and sources of added sugar in Indonesia: a review. Asia Pac J Clin Nutr. https://doi.org/10.6133/apjcn.042017.07
Haning MTAA., Muqni AD (2016) The government policy relating to sugar-sweetened beverages in Indonesia. Indian J Community Health 28(3):222–227
Booth SL, Sallis JF, Ritenbaugh C, Hill JO, Birch LL, Frank LD, Glanz K, Himmelgreen DA, Mudd M, Popkin BM, Rickard KA, St Jeor S, Hays NP (2001) Environmental and societal factors affect food choice and physical activity: rationale, influences, and leverage points. Nutr Rev 59(3 Pt 2):S21–S39 (discussion S57–S65)
Brooks CJ, Gortmaker SL, Long MW, Cradock AL, Kenney EL (2017) Racial/ethnic and socioeconomic disparities in hydration status among US adults and the role of tap water and other beverage intake. Am J Public Health 107(9):1387–1394. https://doi.org/10.2105/AJPH.2017.303923
Soares LC, Griesinger MO, Dachs JN, Bittner MA, Tavares S (2002) Inequities in access to and use of drinking water services in Latin America and the Caribbean. Rev Panam Salud Publica 11(5–6):386–396
Han E, Powell LM (2013) Consumption patterns of sugar-sweetened beverages in the United States. J Acad Nutr Diet 113(1):43–53. https://doi.org/10.1016/j.jand.2012.09.016
Mazarello Paes V, Hesketh K, O’Malley C, Moore H, Summerbell C, Griffin S, van Sluijs EM, Ong KK, Lakshman R (2015) Determinants of sugar-sweetened beverage consumption in young children: a systematic review. Obes Rev 16(11):903–913. https://doi.org/10.1111/obr.12310
Moreira NF, da Veiga GV, Santaliestra-Pasias AM, Androutsos O, Cuenca-Garcia M, de Oliveira ASD, Pereira RA, de Moraes ABV, Van den Bussche K, Censi L, Gonzalez-Gross M, Canada D, Gottrand F, Kafatos A, Marcos A, Widhalm K, Molnar D, Moreno LA (2018) Clustering of multiple energy balance related behaviors is associated with body fat composition indicators in adolescents: results from the HELENA and ELANA studies. Appetite 120:505–513. https://doi.org/10.1016/j.appet.2017.10.008
Gubbels JS, Kremers SP, Stafleu A, de Vries SI, Goldbohm RA, Dagnelie PC, de Vries NK, van BS, Thijs C (2011) Association between parenting practices and children’s dietary intake, activity behavior and development of body mass index: the KOALA Birth Cohort Study. Int J Behav Nutr Phys Act 8:18. https://doi.org/10.1186/1479-5868-8-18
Hobbs M, Pearson N, Foster PJ, Biddle SJ (2015) Sedentary behaviour and diet across the lifespan: an updated systematic review. Br J Sports Med 49(18):1179–1188. https://doi.org/10.1136/bjsports-2014-093754
Acknowledgements
Participant recruitment and data collection in all countries was performed by IPSOS.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Informed consent
All the participants gave their consent prior the inclusion in the study. All data were recorded anonymously.
Ethical standards
The protocol of the surveys was reviewed and approved by the Institutional Review Board, Office of Research Compliance of the University of Arkansas (IRB Protocol # 14-12-376).
Conflict of interest
CM, RB, JB and IG are full-time employees of Danone Research. JS-S, LAM, SAK, JG and HM are members of the advisory board on fluid intake of Danone Research, and have received consultancies from Danone Research. SAK was a scientific consultant for Quest Diagnostics and has active research grants from Danone Research. JS-S and LAM has received consultancies from Danone S.A.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Morin, C., Gandy, J., Brazeilles, R. et al. Fluid intake patterns of children and adolescents: results of six Liq.In7 national cross-sectional surveys. Eur J Nutr 57 (Suppl 3), 113–123 (2018). https://doi.org/10.1007/s00394-018-1725-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-018-1725-y