
Abstract
Background
Reperfusion of the infarct related artery (IRA) prior to PCI is prognostically important in patients with acute ST segment elevation myocardial infarction (STEMI). Reperfusion is either achieved spontaneously, facilitated by GP IIb/ IIIa inhibitors, or mechanically by crossing the guide wire beyond the lesion. In order to test the hypothesis that a visible coronary anatomy is independently associated with procedural and clinical outcomes, we evaluated the frequency and prognostic impact of guide wire facilitated reperfusion of the IRA before primary PCI.
Methods and results
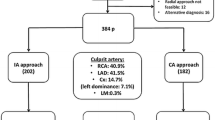
We enrolled 311 consecutive patients with successful primary PCI for STEMI (TIMI grade ≥2 flow) within 12 h after onset of symptoms. Among these, 90 patients (28.9%) had a spontaneously reperfused IRA on initial angiogram, 56 patients (18.0%) achieved reperfusion after crossing of the guide wire, and 165 patients (53.1%) successful reperfusion only after PCI. Variables associated with successful guide wire facilitated reperfusion were younger age, no history of arterial hypertension, active smoking status, negative cardiac troponin T on admission, and an infarct in the territory of the right coronary artery. Patients with spontaneous reperfusion or reperfusion after crossing of the guide wire required less fluoroscopic time and less contrast material during angiography and had higher procedural success rates (TIMI grade 3 flow 91.1 vs 79.4%, p=0.048) than patients without initial reperfusion. In addition, patients with reperfusion after crossing the lesion with the guide wire had lower mortality rates at 30 days (3.6 vs 9.1%) and after a median of 16 months (3.6 vs 13.9%, p=0.03) than those with reperfusion after PCI.
Conclusions
Reperfusion of an occluded IRA by crossing the guide wire is associated with higher procedural success rates and better outcomes. Better roadmapping and device selection represent potential reasons but the exact mechanism for these benefits is still illusive.
Similar content being viewed by others

References
Ross AM, Coyne KS, Moreyra E et al (1998) Extended mortality benefit of early postinfarction reperfusion. GUSTO-I Angiographic Investigators. Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries Trial. Circulation 97:1549–1556
Brodie BR, Stuckey TD, Hansen C, Muncy D (2000) Benefit of coronary reperfusion before intervention on outcomes after primary angioplasty for acute myocardial infarction. Am J Cardiol 85:13–18
Stone GW, Cox D, Garcia E et al (2001) Normal flow (TIMI-3) before mechanical reperfusion therapy is an independent determinant of survival in acute myocardial infarction. Analysis from the Primary Angioplasty in Myocardial Infarction trials. Circulation 104:636–641
Brener SJ, Barr LA, Burchenal JE et al (1998) A randomized, placebo-controlled trial of platelet glycoprotein IIb/IIIa blockade with primary angioplasty for acute myocardial infarction. 2b/3a blocker and Primary PTCA Organization and Randomized Trial. Circulation 98:734–741
Montalescot G, Borentain M, Payot L et al (2004) Early vs late administration of glycoprotein IIb/IIIa inhibitors in primary percutaneous coronary intervention of acute ST-segment elevation myocardial infarction. A meta-analysis. JAMA 292:362–366
Berger PB, Ellis SG, Holmes DR et al (1999) Relationship between delay in performing direct coronary angioplasty and early clinical outcome in patients with acute myocardial infarction. Circulation 100:14–20
Brodie BR, Stuckey TD, Wall TC et al (1998) Importance of time to reperfusion for 30-day and late survival and recovery of left ventricular function after primary angioplasty for acute myocardial infarction. J Am Coll Cardiol 1312–1319
Cannon CP, Gibson CM, Lambrew CT et al (2000) Relationship of symptom- onset-to-balloon time and doorto- balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA 283:2941–2947
Cannon CP, Gibson CM, Lambrew CT et al, for the NRMI 2 and 3 Investigators (2000) Longer thrombolysis door-to-needle times are associated with increased mortality in acute myocardial infarction. An analysis of 85 589 patients in the National Registry of Myocardial Infarction 2+3. J Am Coll Cardiol 35(Suppl A):376A
Antman EM, Giugliano RP, Gibson CM et al, for the Thrombolysis in Myocardial Infarction (TIMI) 14 Investigators (1999) Abciximab facilitates the rate and extent of thrombolysis. Results of TIMI 14 trial. Circulation 99:2720–2732
Ross AM, Coyne KS, Reiner JS et al (1999) A randomized trial comparing primary angioplasty with a strategy of short-acting thrombolysis and immediate planned rescue angioplasty in acute myocardial infarction. The PACT trial. PACT investigators. Plasminogen- activator Angioplasty Compatibility Trial. J Am Coll Cardiol 34:1954–1962
Clements IP, Christian TF, Higano ST et al (1993) Residual flow to the infarct zone as a determinant of infarct size after direct angioplasty. Circulation 88:1527–1533
Hatada K, Sugiura T, Kamihata H et al (2001) Clinical significance of coronary flow to the infarct zone before successful primary percutaneous transluminal coronary angioplasty in acute myocardial infarction. Chest 120:1959–1963
Meyborg P, Abdel-Wahab M, Herrmann G, Geist V, Khattab AA, Kruger D, Lins M, Toelg R, Simon R, Richardt G (2006) Relationship between therapeutic time intervals and intermediate term left ventricular systolic function in patients treated with facilitated percutaneous coronary intervention for acute myocardial infarction. Clin Res Cardiol Dec 14; Epub ahead
The TIMI Study Group (1985) The Thrombolysis in Myocardial Infarction (TIMI) trial: phase 1 findings. N Engl J Med 312:932–936
Müller-Bardorff M, Freitag H, Scheffold T et al (1995) Development and characterization of a rapid assay for bedside determinations of cardiac troponin T. Circulation 92:2869–2875
Ohman EM, Armstrong PW, White HD et al, for the GUSTO-III Investigators (1999) Risk stratification with a point-of-care cardiac troponin T test in acute myocardial infarction. Am J Cardiol 84:1281–1286
Stubbs P, Collinson P, Moseley D et al (1996) The prognostic significance of admission troponin T concentrations in myocardial infarction. Circulation 94:1291–1297
Giannitsis E, Lehrke S, Wiegand U et al (2000) Risk stratification in patients with inferior acute myocardial infarction treated by percutaneous coronary interventions. Circulation 102:2038–2044
Matetzky S, Sharir T, Domingo M et al (2000) Elevated troponin I level on admission is associated with adverse outcome of primary angioplasty in acute myocardial infarction. Circulation 102:1611–1616
Frostfeldt G, Gustafsson G, Lindahl B et al (2001) Possible reasons for the prognostic value of troponin-T on admission in patients with ST-elevation myocardial infarction. Coron Artery Dis 12:227–237
Ellis SG, Topol EJ, Gallison L et al (1988) Predictors of success for coronary angioplasty performed for acute myocardial infarction. J Am Coll Cardiol 12:1407–1415
Cura FA, L'Allier PL, Kapadia SR et al, for the GUSTO IIb and RAPPORT Investigators (2001) Predictors and prognosis of suboptimal coronary blood flow after primary coronary angioplasty in patients with acute myocardial infarction. Am J Cardiol 88:124–128
Frey N, Dietz A, Kurowski V et al (2001) Angiographic correlates of a positive troponin T test in patients with unstable angina. Crit Care Med 29:1130–1136
Giannitsis E, Bardorff MM, Schweikart S et al (2000) Relationship of cardiac troponin T and procoagulant activity in unstable angina. Thromb Haemost 83:224–228
Gibson CM, de Lemos JA, Murphy SA et al, for the TIMI Study Group (2001) Combination therapy with abciximab reduces angiographically evident thrombus in acute myocardial infarction: a TIMI 14 substudy. Circulation 103:2550–2554
Giannitsis E, Müller Bardorff M, Lehrke S et al (2001) Admission troponin T level predicts clinical outcomes, TIMI flow, and myocardial tissue perfusion after primary percutaneous intervention for acute STsegment elevation myocardial infarction. Circulation 104:630–635
Lehrke S, Giannitsis E, Katus HA (2004) Admission troponin T, advanced age and male gender identify patients with improved myocardial tissue perfusion after abciximab administration for ST-segment elevation myocardial infarction. Thromb Haemost 92:1214–1220
Hasdai D, Lerman A, Rihal CS et al (1999) Smoking status and outcome after primary coronary angioplasty for acute myocardial infarction. Am Heart J 137:612–620
The GUSTO V Investigators (2001) Reperfusion therapy for acute myocardial infarction with fibrinolytic therapy or combination reduced fibrinolytic therapy and platelet glycoprotein IIb/IIIa inhibition: the GUSTO V randomised trial. Lancet 357:1905– 1914
Montalescot G, Barragan P, Wittenberg O et al, for the ADMIRAL Investigators (2001) Platelet glycoprotein IIb/IIIa inhibition with coronary stenting for acute myocardial infarction. N Engl J Med 344:1895–1903
Neumann FJ, Blasini R, Schmitt C et al (1998) Effect of glycoprotein IIb/ IIIa receptor blocker on recovery of coronary flow and left ventricular function after the placement of coronary- artery stents in acute myocardial infarction. Circulation 98:2695–2701
Author information
Authors and Affiliations
Corresponding author
Additional information
V. Kurowski and E. Giannitsis equally as first authors
Rights and permissions
About this article
Cite this article
Kurowski, V., Giannitsis, E., Killermann, D.P. et al. The effects of facilitated primary PCI by guide wire on procedural and clinical outcomes in acute ST-segment elevation myocardial infarction. Clin Res Cardiol 96, 557–565 (2007). https://doi.org/10.1007/s00392-007-0532-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-007-0532-x