
Summary.
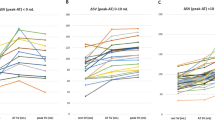
Exercise training for patients with coronary artery disease (CAD) is recommended in a wide range between 40–85% of maximum functional capacity (MFC) or 55–90% of maximum heart rate (HR). During exercise, high levels of catecholamines and metabolic acidosis could induce arrhythmia and ischemia. But catecholamines have never been determined in CAD during constant load exercise in the upper range of recommended intensities. In 11 CAD patients (age 58±8 years, BMI 26.1±4.0kg·m–2, NYHA I n=7, II n=4) we tested the maximum functional capacity (MFC), norepinephrine (NE), epinephrine (E) and blood lactate ([Lac–]B) in a symptom-limited incremental ergometer test. Related to the exercise recommendation, the kinetics of NE, E and [Lac–]B were determined in two 30min constant load tests in randomized order: one was performed at the anaerobic lactate threshold (CTAT), a second was performed 10% above the individual threshold intensity (CT+10%). In the incremental tests maximum workload and VO2 were 141±54 W and 1766±532 ml·min–1, respectively (85±22% of normal; [Lac–]B 5.7±1.9mmol·l–1, HR 138±28b·min–1, NE 11.7±5.1, E 1.6±1.4nmol·l–1). In CTAT the anaerobic threshold (63±7% of MFC) represented the mean range of recommended exercise intensity for CAD (40–85%) and could be validated as steady-state intensity because catecholamines and [Lac–]B concentrations remained constant after the initial increase (workload 88±35W, [Lac–]B 3.3±1.4 mmol·l–1, HR 117± 23b·min–1, NE 8.3±3.5, E 0.8± 0.7nmol·l–1). In all patients CT+10% (71±7% of MFC) led to a continous rise in [Lac–]B, to a NE overload and to earlier exhaustion, although the intenisties were in the recommended training range (workload 100±38W, [Lac–]B 5.8± 1.9mmol·l–1, HR 129± 29b·min–1, NE 13.9±6.9, E 1.5± 1.7nmol·l–1; p<0.01 against CTAT for all except E). Conclusions In the upper range of recommended training intensity for CAD patients, norepinephrine and lactate were higher during endurance exercise than at MFC in incremental tests. Endurance exercise with intensities >70% of MFC could overload the cardiac patient and increase the risk of arryhthmia and ischemia. Therefore, endurance exercise should be performed below 70% of MFC or below 85% of maximum HR, respectively, whereas higher intensities should apply to interval exercise.
Zusammenfassung.
Ausdauerbelastungen für Patienten mit koronarer Herzkrankheit sind bei 55–90% der maximalen Herzfrequenz oder 40–85% der maximalen Leistung empfohlen. Steuergröße von Metabolismus und Herz-Kreislauf sowie Trigger myokardialer Ischämien und Herzrhythmusstörungen sind u.a. die Plasmakatecholamine. Fragestellung war daher, ob Plasmakatecholamine bei Dauerbelastungen an bzw. oberhalb der anaeroben Schwelle den Bereich des Steady-States markieren bzw. übersteigen, und ob die weitgefassten Belastungsempfehlungen mit Vorgaben korrelieren, die sich aus dem Katecholaminverhalten bei den Dauertests ableiten? Bei 11 Patienten mit koronarer Herzkrankheit wurde die anaerobe Schwelle im doppelten Ergometerstufentest ermittelt. In zwei Dauertests über 30min mit und 10% oberhalb dieser Schwellenintensität wurde das Katecholamin-, Stoffwechsel- und Atmungsverhalten bestimmt. Bei einer maximalen Stufentestleistung von 141±54 W bzw. VO2max von 1766±532 ml·min–1 entsprechend 85±22% des Normwertes stiegen Adrenalin und Noradrenalin auf 1,6±1,4 bzw. 11,7±5,1nmol·l–1 an. In den Dauertests über 30min mit der Intensität der anaeroben Schwelle bei 88±35 W stellte sich ein Steady-State von Laktat (3,3±1,4mmol·l–1), Adrenalin (0,8±0,7nmol·l–1) und Noradrenalin (8,3±3,5nmol·l–1) ein. In den überschwelligen Dauertests mit 100±38 Watt stiegen Laktat (5,8±1,9mmol·l–1), Adrenalin (1,5±1,7nmol·l–1) und Noradrenalin (13,9±6,9nmol·l–1) stetig an und führten zum Belastungsabbruch nach 19,2±2,7min (p<0,001). Überschwellige Dauerbelastungen bei 71% der Maximalleistung führten zu 18% höheren Plasmanoradrenalinwerten als am Ende eines symptomlimitierten Belastungs-EKGs. Damit verbunden waren Ermüdungsanstiege metabolischer und kardiopulmonaler Größen und vorzeitige Erschöpfung. Mit der Dauerleistung im maximalen Laktat-Steady-State bei 63% der Maximalleistung korreliert eine Belastung bei 70% der Herzfrequenzreserve bzw. eine Belastung bei 85% der symptomlimitierten Herzfrequenz besser als die methodisch aufwendigeren Verfahren der Ventilations- und fixen Laktatschwellen.
Similar content being viewed by others


Author information
Authors and Affiliations
Additional information
Eingegangen: 25. Februar 2002 Akzeptiert: 31. Juli 2002
Correspondence to Uwe Tegtbur
Rights and permissions
About this article
Cite this article
Tegtbur, U., Meyer, H., Machold, H. et al. Belastungsdiagnostische Kenngrößen und Katecholamine bei Koronarpatienten. Z Kardiol 91, 927–936 (2002). https://doi.org/10.1007/s00392-002-0867-2
Issue Date:
DOI: https://doi.org/10.1007/s00392-002-0867-2