
Abstract
Objective
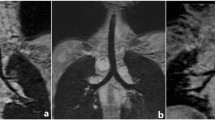
The role of preoperative contrast-enhanced computerized tomography (CT) of chest with three-dimensional (3D) reconstructions was evaluated in neonates with esophageal atresia and tracheoesophageal fistula.
Methods
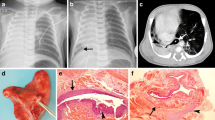
This was a prospective study which investigated 30 cases of esophageal atresia with tracheoesophageal fistula. All patients were evaluated preoperatively with contrast-enhanced spiral CT using a low-dose CT protocol. 3D CT reconstruction images were evaluated for the type of esophageal atresia, the distance between the upper and lower esophageal pouches, origin, level and position of the fistula, and the presence or absence of any other cardiac, pulmonary or mediastinal lesions and the findings were correlated with the findings at surgery. The radiation dose for each patient was calculated using the formula—Effective dose (E) = DLP × (E/DLP)age.
Results
All the 30 cases had type-C esophageal atresia with tracheoesophageal fistula as per Gross classification. The exact site of the fistula could be identified only in 26 (80 %) cases. The mean gap between the upper pouch and lower fistula was 0.95 ± 0.57 cm (range 0.2–2.8 cm) on CT scan and 1.38 ± 0.61 cm (range 0.5–3.2 cm) at surgery. On statistical analysis, the correlation was found to be significant (p < 0.0001). In addition, lung pathology (consolidation), cardiac pathology and vertebral anomaly were also detected on CT scan in some cases. The mean radiation dose for the neonates who underwent CT chest was calculated to be 1.79 mSv which is significantly high.
Conclusion
Though preoperative CT scan of chest has many advantages, it involves significant exposure to ionizing radiation and risk of radiation-induced cancer in the future. Additionally in 20 % of cases, the fistula could not be located on CT scan. The most common variety of esophageal atresia and tracheoesophageal fistula is Gross type C (86 %) that has low to intermediate gap (97 %) and can be anastomosed primarily. Thus, CT scan can provide good anatomical delineation, but may not help in surgical decision making. Hence, performing CT in these cases would unnecessarily expose the neonates to ionizing radiation. Therefore, there is no role for CT scan in the routine preoperative assessment of EA with distal TEF.


Similar content being viewed by others

References
Harmon CM, Coran AG (2006) Congenital anomalies of esophagus. In: Grosfeld JL, O’Neill JA, Fronkalsrud EW, Coran AG (eds) Pediatric surgery. Mosby-Elsevier, Philadelphia, pp 1051–1082
Bax KN, Roskott AMC, Vander Zee DC (2008) Esophageal atresia without distal tracheoesophageal fistula: high incidence of proximal fistula. J Pedaitr Surg 43:522–525
Guo W, Li Y, Jiao A, Peng Y, Hou D, Chen Y (2010) Tracheoesophageal fistula after primary repair of type C esophageal atresia in the neonatal period: recurrent or missed second congenital fistula. J Pediatr Surg 45:2351–2355
Islam S, Cavanaugh E, Honeke R, Hirschl RB (2004) Diagnosis of proximal tracheoesophageal fistula using three-dimensional CT scan: a case report. J Pediatr Surg 39(1):100–102
Gross RE (1953) The surgery of infancy and childhood. WB Saunders, Philadelphia
Huda W (2007) Radiation doses and risks in chest computed tomography examinations. Proc Am Thorac Soc 4:316–320
Shrimpton PC, Hillier MC, Lewis MA, Dunn M (2006) National survey of doses from CT in the UK: 2003. Br J Radiol 79:968–980
Chapple CL, Willis S, Frame J (2002) Effective dose in pediatric computed tomography. Phys Med Biol 47:107–115
Brown AK, Tam PK (1996) Measurement of gap length in esophageal atresia: a simple predictor of outcome. J Am Coll Surg 182:41–45
Upadhyaya VD, Gangopadhyaya AN, Gupta DK, Sharma SP, Kumar V et al (2007) Prognosis of congenital tracheoesophageal fistula with esophageal atresia on the basis of gap length. Pediatr Surg Int 23:767–771
Van der Zee DC, Vieirra-Travassos D, De Jong JR, Tytgat SH (2008) A novel technique for risk calculation of anastomotic leakage after thoracoscopic repair for esophageal atresia with distal fistula. World J Surg 32:1396–1399
Rossi C, Domini M, Aquino A, Pesico A, Lelli-Chiesa P (1998) A simple and safe method to visualize the inferior pouch in esophageal atresia without fistula. Pediatr Surg Int 13:535–536
Koplewitz BZ, Udassin R (2003) Radiographic assessment of the gap between oesophageal pouches in infants with oesophageal atresia without fistula. Eur J Pediatr 162:650–651
Atzori P, Iacobelli BD, Bottero S et al (2006) Preoperative tracheobronchoscopy in new borns with esophageal atresia: does it matter? J Pediatr Surg 41(6):1054–1056
de Blic J, Marchac V, Scheinmann P (2002) Complications of flexible bronchoscopy in children: prospective study in 1,328 procedures. Eur Respir J 20:1271–1276
Ianolli ED, Litman RS (2002) Tension pneumothorax during flexible fiberoptic bronchoscopy in a newborn. Anesth Analg 94:512–513
Garcia NM, Thompson JW, Shaul DB (1998) Definitive localization of isolated tracheoesophageal fistula using bronchoscopy and esophagoscopy for guide wire placement. J Pediatr Surg 33:1645–1647
Chang KL, Saing H (1995) Combined flexible endoscopy and fluoroscopy in assessment of gap between the two esophageal pouches in esophageal atresia without fistula. J Pediatr Surg 30(5):668–670
Johnson JF, Sueoka BL, Mulligan ME, Lugo EJ (1985) Tracheoesophageal fistula: diagnosis with CT. Pediatr Radiol 15:134–135
Tam PKH, Chan FL, Saing H (1987) Diagnosis and evaluation of esophageal atresia by direct sagittal CT. Pediatr Radiol 17:68–70
Ratan SK, Varshney A, Sumita M, Saxena NC, Kakar S, Sodhi PK (2004) Evaluation of neonates with esophageal atresia using chest CT scan. Pediatr Surg Int 20:757–761
Lam WWK, Tam PKH, Chan FL, Chan KL, Cheng W (2000) Esophageal atresia and tracheal stenosis: use of three-dimensional CT and virtual bronchoscopy in neonate, infants and children. AJR Am J Roentgenol 174:1009–1012
Fitoz S, Atasoy C, Yagmurlu A, Akyar S, Erden A, Dindar H (2000) Three-dimensional CT of congenital esophageal atresia and distal tracheoesophageal fistula in neonates: preliminary results. AJR Am J Roentgenol 175:1403–1407
Beasley S (2009) Congenital malformation. In: Parikh DH, Crabbe DCG, Auldist AW, Rothenberg SS (eds) Pediatric thoracic surgery. Springer, London, pp 281–309
National Academy of Sciences Committee on the Biological Effects of Ionizing Radiation (2005) Report VII (BEIR VII, Phase 2): health risks from exposure to low levels of ionizing radiation. National Research Council, Washington. http://books.nap.edu/catalog/11340.html
Brenner DJ, Elliston CD, Hall EJ et al (2001) Estimated risks of radiation induced fatal cancer from pediatric CT. Am J Roentgenol 176:289–296
United Nations Scientific Committee on the Effects of Atomic radiation (UNSCEAR) (2000) Sources and effects of ionizing radiation. United Nations, New York
Piccolo RL, Bongini U, Basile M, Savelli S et al (2012) Chest fast MRI: an imaging alternative on preoperative evaluation of pectus excavatum. J Pediatr Surg 47:485–489
Acknowledgments
We would like to thank Dr. Dhananjay Vaze, senior registrar, Pediatric Surgery, PGIMER, Chandigarh, for his invaluable effort for helping in editing the manuscript and few vital suggestions.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mahalik, S.K., Sodhi, K.S., Narasimhan, K.L. et al. Role of preoperative 3D CT reconstruction for evaluation of patients with esophageal atresia and tracheoesophageal fistula. Pediatr Surg Int 28, 961–966 (2012). https://doi.org/10.1007/s00383-012-3111-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-012-3111-9