
Abstract
Introduction
Given the large number of cerebral palsy patients who have undergone selective dorsal rhizotomy in the past two decades, it is clearly imperative that the clinical community be provided with objective and compelling evidence of the long-term sequelae of the procedure.
Materials and methods
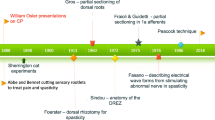
In the early 1980s, Peacock in Cape Town shifted the site of the rhizotomy from the conus medullaris to the cauda equina, and in the past 25 years, more than 200 children have been operated on. We have studied the incidence of spinal deformities after multiple-level laminectomy and recorded a 20% incidence of isthmic spondylolysis or grade-I spondylolisthesis. We have also conducted a long-term prospective gait analysis study on a cohort of 14 ambulatory patients who were operated on in 1985.
Results
Ten years after surgery, our patients had increased ranges of motion that were within normal limits. Step length was significantly improved, although cadence was unchanged postoperatively and was significantly less than normal age-matched control subjects.
Discussion
We have recently tracked down all 14 patients from the original cohort and are currently completing a 20-year prospective follow-up analysis of their neuromuscular function and gait. Our preliminary data suggest that selective dorsal rhizotomy is not only an effective method for alleviating spasticity but it also leads to long-term functional benefits.


Similar content being viewed by others


References
Abbott R, Forem SL, Johann M (1989) Selective posterior rhizotomy for the treatment of spasticity: a review. Child’s Nerv Syst 5:337–346
Aiona MD, Sussman MD (2004) Treatment of spastic diplegia in patients with cerebral palsy: Part II. J Pediatr Orthop B 13:S13–S38
Berman B (1989) Selective posterior rhizotomy: does it do any good? Neurosurg State Art Rev 4:431–444
Berman B, Vaughan CL, Peacock WJ (1990) The effect of rhizotomy on movement in patients with cerebral palsy. Am J Occup Ther 44:511–516
Fasano VA, Barolat-Romana G, Ivaldi A, Sguazzi A (1976) La radicotomie postérieure fonctionnelle dans le traitement de la spasticité cérébrale. Neurochirurgie 22:23–34
Foerster O (1913) On the indications and results of the excision of posterior nerve roots in men. Surg Gynecol Obstet 6:463–474
Gros C, Ouaknine G, Vlahovitch B, Frerebeau P (1967) La radicotomie sélective postérieure dans le traitment neuro-chirurgical de l’hypertonie pyramidale. Neurochirurgie 13:505–518
Hof AL (1996) Scaling gait data to body size. Gait Posture 4:222–223
Kim DS, Choi JU, Yang KH, Park CI, Park ES (2002) Selective posterior rhizotomy for lower extremity spasticity: how much and which of the posterior rootlets should be cut? Surg Neurol 57:87–93
Klingbeil H, Baer HR, Wilson PE (2004) Aging with a disability. Arch Phys Med Rehabil 85:S68–S73
McLaughlin JF, Bjornson KF, Astley SJ, Hays RM, Hoffinger SA, Armantrout EA, Roberts TS (1994) The role of selective dorsal rhizotomy in cerebral palsy: critical evaluation of a prospective clinical series. Dev Med Child Neurol 36:755–769
Oppenheim WL (1990) Selective posterior rhizotomy for spastic cerebral palsy. A review. Clin Orthop Relat Res Apr(253):20–29
Park TS (2000) Selective dorsal rhizotomy: an excellent therapeutic option for spastic cerebral palsy. Clin Neurosurg 47:422–439
Park TS, Owen JH (1992) Surgical management of spastic diplegia in cerebral palsy. N Engl J Med 326:745–749
Peacock WJ, Eastman RW (1981) The neurosurgical management of spasticity. S Afr Med J 60:849–850
Peter JC, Hoffman EB, Arens LJ, Peacock WJ (1990) Incidence of spinal deformity in children after multiple level laminectomy for selective posterior rhizotomy. Child’s Nerv Syst 6:30–32
Peter JC, Hoffman EB, Arens LJ (1993) Spondylolysis and spondylolisthesis after five-level lumbosacral laminectomy for selective posterior rhizotomy in cerebral palsy. Child’s Nerv Syst 9:285–287
Russell D, Rosenbaum P, Cadman D, Gowland C, Hardy S, Jarvis S (1989) The Gross Motor Function Measure: a means to evaluate the effects of physical therapy. Dev Med Child Neurol 31:341–352
Steinbok P (2001) Outcomes after selective dorsal rhizotomy for spastic cerebral palsy. Child’s Nerv Syst 17:1–18
Subramanian N, Vaughan CL, Peter JC, Arens LJ (1998) Gait before and 10 years after rhizotomy in children with cerebral palsy spasticity. J Neurosurg 88:1014–1019
Vaughan CL, Berman B, Peacock WJ (1991) Cerebral palsy and rhizotomy. A 3-year follow-up evaluation with gait analysis. J Neurosurg 74:178–184
Vaughan CL, Berman B, Peacock WJ, Eldridge NE (1989) Gait analysis and rhizotomy: past experience and future considerations. Neurosurg State Art Rev 4:445–458
Vaughan CL, Berman B, Staudt LA, Peacock WJ (1988) Gait analysis of cerebral palsy children before and after rhizotomy. Pediatr Neurosci 14:297–300
Vaughan CL, Subramanian N, Busse ME (1998) Selective dorsal rhizotomy as a treatment option for children with spastic cerebral palsy. Gait Posture 8:43–59
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Langerak, N.G., Lamberts, R.P., Fieggen, A.G. et al. Selective dorsal rhizotomy: long-term experience from Cape Town. Childs Nerv Syst 23, 1003–1006 (2007). https://doi.org/10.1007/s00381-007-0383-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-007-0383-9