
Abstract
Objective
The objective was to review the clinical aspects and therapeutic strategies in a series of aneurysmal vasculopathies seen in children 15 years or under.
Methods
From our dedicated neurovascular databank of patients, we reviewed 59 consecutive children who had 75 separate lesions.
Results
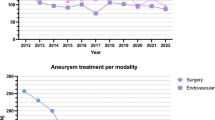
The children were divided into four age groups: below 2 years (22%), 2–5 years (24%), 6–10 years (24%) and 11–15 years (30%). Thirty-three children had dissecting aneurysms, 2 had chronic post-traumatic aneurysms, 8 had infectious aneurysms and 16 had saccular lesions. Twenty-seven percent of the lesions were in the posterior circulation, and 21% developed on the middle cerebral artery. Most dissecting lesions were encountered in the vertebrobasilar system, while saccular lesions were present mostly in the anterior circulation. Half of all cases presented with haemorrhage. Haemorrhage in patients below 2 years of age was due to dissecting aneurysms, while saccular aneurysms were responsible for haemorrhage in patients above 5 years of age. Five children had familial disease and 9 presented with multiple aneurysms. Forty-eight children were referred to us for treatment. Thirty-two underwent surgical (21.9%), endovascular (62.8%) or combined (9.3%) treatment. Eleven patients were treated conservatively and in 5 patients the aneurysms had spontaneously thrombosed at admission. Overall, complete or partial spontaneous thrombosis was seen in 10 patients (16.9%). Dissecting aneurysms were frequent in children of all ages with either associated thrombosis or arterial tear with repeated acute haemorrhage and poor outcome. Two types of dissection seem identifiable despite the small number of cases collected: acute segmental arterial tear without thrombosis, acute subarachnoid haemorrhage (SAH) and recurrence before 5 years; and subacute focal dissection with partial thrombosis (or mural haematoma), rare SAH and no early recurrence. The former would require aggressive management whereas the latter often do not require interventional approaches. The mortality in our series of aneurysms is low in the treated group (10.42%). The overall tolerance to haemorrhage seems better than in adults, as already stressed in the literature.
Conclusion
The multiple etiologies encountered confirm the heterogenous nature of “aneurysms”. The variety of treatments used suggests the need to categorise aneurysms into subgroups in sufficient numbers to fully appreciate the behavior of the lesions and make the appropriate therapeutic decisions.




Similar content being viewed by others

References
Chen YL, Luo CB, Hsu SW, Rodesch G, Lasjaunias P (2001) Tuberous sclerosis complex with an unruptured intracranial aneurysm: manifestation of contiguous gene syndrome. Interv Neuroradiol 7:337–341
Chul Suh D, Alvarez H, Sainte Rose C, Lasjaunias P (2001) Supraclinoid internal carotid arterial aneurysm presenting as a suprasellar mass-like lesion in a child. Interv Neuroradiol 7:357–361
De Blasi R, Lasjaunias P, Rodesch G, Alvarez H (1997) Endovascular treatment of a ruptured intracranial arterial aneurysm in a 12-year-old child with recessive polycystic kidney disease. Interv Neuroradiol 3:333–336
Lasjaunias P (1999) Segmental identity and vulnerability. Interv Neuroradiol 6:113–124
Lasjaunias P (2000) From aneurysm to aneurysmal vasculopathies. Interv Neuroradiol 5:105–108
Lasjaunias P, Campi A, Rodesch G, Alvarez H, Kanaan I, Taylor W (1997) Aneurysmal disease in children: review of 20 cases with intracranial arterial localizations. Interv Neuroradiol 3:215–229
Laughlin S, Ter Brugge KG, Willinsky RA, Armstrong DC, Montanera WJ, Humphreys RP (1997) Endovascular management of pediatric intracranial aneurysms. Interv Neuroradiol 3:205–214
Lenthall RK, Cinalli G, Rodesch G, Lasjaunias P (1999) Endovascular management of a traumatic basilar tip aneurysm following endoscopic ventriculostomy in a child. Interv Neuroradiol 5:57–60
Locksley HB (1966) Report on the cooperative study of intracranial aneurysms and subarachnoid hemorrhage. Section V. 1. Natural history of subarachnoid hemorrhage, intracranial aneurysms and arteriovenous malformations. Based on 6368 cases in cooperative study. J Neurosurg 25:219–239
Luo CB, Chen YL, Hsu SW, Alvarez H, Rodesch G, Lasjaunias P (2001) Spontaneous healing and complete disappearance of a giant basilar tip aneurysm in a child. Interv Neuroradiol 7:141–145
Meyer FB, Sundt TM Jr, Fode NC, Morgan MK, Forbes GS, Mellinger JF (1989) Cerebral aneurysms in childhood and adolescence. J Neurosurg 70:420–425
Ostergaard JR (1991) Aetiology of intracranial saccular aneurysms in children. Br J Neurosurg 5:575–580
Ostergard JR, Voldby B (1983) Intracranial arterial aneurysms in children and adolescents. J Neurosurg 58:832–837
Pasqualin A, Mazza C, Cavazzani P, Scienza R, Da Pian R (1986) Intracranial aneurysms and subarachnoid hemorrhage in children and adolescents. Childs Nerv Syst 2:185–190
Proust F, Toussaint P, Garnieri J, Hannequin D, Legars D, Houtteville JP, Freger P (2001) Pediatric cerebral aneurysms. J Neurosurg 94:733–739
Schubiger O, Valavanis A, Wichmann W (1987) Growth-mechanism of giant intracranial aneurysms; demonstration by CT and MR imaging. Neuroradiology 29:266–277
Sedat J, Alvarez H, Rodesch G, Lasjaunias P (1999) Multifocal cerebral fusiform aneurysm in children with immune deficiencies: report on four cases. Interv Neuroradiol 5:151–156
Tan MP, McConachie NS, Vloeberghs M (1998) Ruptured fusiform aneurysm in a neonate. Childs Nerv Syst 14:467–469
Acknowledgements
We are particularly indebted to S. Cullen, MD, for editing this text.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lasjaunias, P., Wuppalapati, S., Alvarez, H. et al. Intracranial aneurysms in children aged under 15 years: review of 59 consecutive children with 75 aneurysms. Childs Nerv Syst 21, 437–450 (2005). https://doi.org/10.1007/s00381-004-1125-x
Received:
Revised:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-004-1125-x