
Abstract
Marine teleost fish secrete bicarbonate (HCO3 −) into the intestine to aid osmoregulation and limit Ca2+ uptake by carbonate precipitation. Intestinal HCO3 − secretion is associated with an equimolar transport of protons (H+) into the blood, both being proportional to environmental salinity. We hypothesized that the H+-sensitive haemoglobin (Hb) system of seawater teleosts could be exploited via the Bohr and/or Root effects (reduced Hb-O2 affinity and/or capacity with decreasing pH) to improve O2 delivery to intestinal cells during high metabolic demand associated with osmoregulation. To test this, we characterized H+ equilibria and gas exchange properties of European flounder (Platichthys flesus) haemoglobin and constructed a model incorporating these values, intestinal blood flow rates and arterial–venous acidification at three different environmental salinities (33, 60 and 90). The model suggested red blood cell pH (pHi) during passage through intestinal capillaries could be reduced by 0.14–0.33 units (depending on external salinity) which is sufficient to activate the Bohr effect (Bohr coefficient of −0.63), and perhaps even the Root effect, and enhance tissue O2 delivery by up to 42 % without changing blood flow. In vivo measurements of intestinal venous blood pH were not possible in flounder but were in seawater-acclimated rainbow trout which confirmed a blood acidification of no less than 0.2 units (equivalent to −0.12 for pHi). When using trout-specific values for the model variables, predicted values were consistent with measured in vivo values, further supporting the model. Thus this system is an elegant example of autoregulation: as the need for costly osmoregulatory processes (including HCO3 − secretion) increases at higher environmental salinity, so does the enhancement of O2 delivery to the intestine via a localized acidosis and the Bohr (and possibly Root) effect.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The marine teleost intestine is a multifunctional organ. It is an important site of digestion, nutrient absorption and metabolic waste excretion in all fishes (Taylor et al. 2011), and in marine teleosts, the intestine is also vital to the absorption of water and excretion of divalent ions (Wilson et al. 2002; Wilson and Grosell 2003). Calcium and magnesium ions in particular are ingested with seawater and, if not dealt with, could accumulate to detrimental levels. This is prevented by their precipitation in carbonate crystals through the secretion of metabolically produced bicarbonate (HCO3 −) into the intestine from epithelial cells lining the lumen (Cooper et al. 2010; Walsh et al. 1991; Wilson et al. 2002; Grosell, 2006, 2011; Wilson and Grosell, 2003; Whittamore et al. 2010).
Although essential to osmoregulation, intestinal HCO3 − secretion also affects the acid–base balance of marine teleosts. The production of HCO3 − from endogenous carbon dioxide (CO2) liberates a proton (H+) that, in order to maintain the intestinal cell’s pH, is extruded basolaterally into the blood (Genz et al. 2008; Grosell et al. 2005; Grosell and Genz 2006; Wilson et al. 2002; Wilson and Grosell 2003) via a sodium-dependent pathway and possible proton pumps (Grosell et al. 2009a, 2009b; Grosell 2010, 2011). Alternatively, the source of HCO3 − in some species or regions of the intestine is transepithelial transfer across both basolateral and apical membranes. However, for either mechanism, the overall effect is quantitatively identical, i.e. a significant blood acidosis in proportion to net HCO3 − secretion rates which are particularly high during enhanced Ca2+ supply to the gut associated with living in hypersaline waters (Genz et al. 2008) or experimental intestinal perfusion with high Ca2+ solutions (Cooper et al. 2010; Whittamore et al. 2010). Furthermore, intestinal HCO3 − production comes with a metabolic cost, as enhanced HCO3 − secretion after a meal has been shown to almost double O2 consumption in the intestinal tissue of gulf toadfish (Opsanus beta) in vitro (Taylor and Grosell 2009). In a situation of high demand for HCO3 − secretion into the intestinal lumen, a mechanism to promote O2 delivery would be beneficial.
Teleost haemoglobins (Hbs) are particularly sensitive to protons, exhibiting some of the largest Bohr effects (reduction in Hb-O2 affinity with a pH reduction) observed in the animal kingdom (Berenbrink et al. 2005). Furthermore, teleost Hbs also exhibit a Root effect, where a reduction in blood pH results in a reduction in blood O2 carrying capacity (Root 1931; Root and Irving 1943). Provided blood pH is reduced during arterial–venous blood transit, these pH-sensitive Hbs allow for enhanced O2 delivery to the tissues. Under steady-state aerobic metabolism, the reduction in blood pH during arterial–venous blood transit arises primarily from metabolically produced CO2. Tissue respiratory quotients (RQ; CO2 produced relative to O2 consumed) are typically 0.7–1.0, and the optimal Bohr coefficient for O2 delivery has been calculated to be ½ of RQ (i.e. a Bohr coefficient of −0.35 to −0.5) (Lapennas 1983), but most teleost fishes have Bohr coefficients in excess of this value (Berenbrink et al. 2005) which could result in an impairment in O2 delivery. Interestingly, in many teleosts with a large Bohr coefficient, the magnitude of the Bohr coefficient is non-linear over different regions of the oxygen equilibrium curve and may be reduced close to this optimal value during some physiological states such as exercise (Brauner et al. 2000b). However, in tissues where arterial–venous blood transit experiences extra acidification in addition to that associated with aerobic metabolism, enhanced O2 delivery can occur via the Bohr/Root effect regardless of the magnitude of the Bohr coefficient. This is the case in the teleost swim bladder and eye, where exceptionally high arterial partial pressures of O2 (PO2) are needed to drive O2 over large diffusion distances and against high hydrostatic pressures (Pelster and Randall 1998).
We hypothesized that a similar O2 delivery mechanism may also take place at the intestine of marine teleosts, where the additional blood acidification associated with secretion of HCO3 − for Ca2+ and Mg2+ precipitation in the gut may exploit a Bohr/Root effect and enhance O2 delivery. It follows that the magnitude of this effect on O2 delivery would increase with salinity. To test these hypotheses, we acclimated European flounder (Platichthys flesus), a species with a well-resolved HCO3 − secretion mechanism, to a number of salinities with the objective of characterizing the Bohr/Root effects of their Hb system. To ascertain this, further experiments were required to estimate the arterial–venous pH change in the capillaries supplying the intestinal cells. As this proved impossible in flounder, in vivo measurements of intestinal venous blood pH using seawater-acclimated rainbow trout (Oncorhynchus mykiss) were performed. From this, it was possible to understand how those Bohr/Root effects might be used to maximize O2 delivery to the intestine during osmoregulation in hyperosmotic environments.
Methods
Fish husbandry
Flounder (Platichthys flesus) (400 ± 64 g) were obtained from Flookburgh, Cumbria, UK. Prior to experiments, fish were maintained in 150-l aerated flow through tanks containing artificial sea water at a salinity of 33 (Tropic Marin Sea Salt, Tropic Marin Centre, UK, added to deionised water) and 12 °C, under a 12-h light:dark photoperiod. Fish were fed weekly on ragworm (Nereis virens), although they were not fed for at least 72 h before experimentation. Fish were anaesthetised (150 mg l−1 of neutralized MS222) and blood was taken via caudal puncture whilst their head was submerged and still showing signs of ventilation. Rainbow trout (Oncorhynchus mykiss; body mass range 506–611 g) were obtained from Hooke Springs Trout Farm, Dorset, and initially held in dechlorinated freshwater. To prepare these fish for subsequent acclimation to seawater they were fed a diet of commercial trout pellets supplemented with increasing amounts of NaCl (Perry et al. 2006; Salman and Eddy, 1990). Dietary salt content was increased in 2 % (w/w) steps every 3–4 days up to a maximum of 12 % (w/w) added NaCl. The external salinity was then gradually raised up to full-strength seawater over a 48-h period and fish were allowed to acclimate for a further 2 weeks prior to use in experiments. All experiments were conducted with the approval of the University of Exeter Ethics Committee and under a UK Home Office license (PPL 30/2217).
Haemolysate preparation
Red blood cells were isolated in whole blood by centrifugation and washed three times in cold Cortland’s physiological saline (8 °C; Wolf, 1963). The red cells were lysed by addition of two times their volume of deionised water (8 °C; Millipore, Direct Q3) and subsequent freezing, and cell debris was removed by 10 min of chilled (4 °C) centrifugation at 14,000 r.p.m. (Thermo Electron Corporation 21000R, Waltham, MA, USA). To remove organic phosphates (ATP and GTP, collectively referred to as NTP) and reduce methaemoglobin levels, sodium dithionite (Sigma-Aldrich) and glycerol were added to haemolysate samples which were then run through two Sephadex PD-10 columns (GE Healthcare Bio-Sciences AB, Uppsala, Sweden) using two separate buffers (deoxygenated 50 mmol l−1 KCl and 50 mmol l−1 Hepes buffers at pH 7.5 and 8.5). To remove the Hepes buffer and further reduce NTP levels (but retain Hb) from the eluted haemolysate, each sample (~1 ml) was placed in a sealed Spectra Por molecular-porous membrane dialysis bag (molecular weight cut-off 6–8 kDa; Spectrum Medical Industries Inc. Los Angeles, USA) and left in 2-l deionised water (Milli-Q) at 5 °C for at least 12 h (deionised water was replaced three times over this period).
Haemoglobin concentration was determined after conversion to cyanomethaemoglobin using a micromolar extinction coefficient of 11 at 540 nm using the Drabkin’s reagent (Sigma-Aldrich) method (Drabkin and Austin 1935), and methaemoglobin content was assessed on identical sub-samples using the spectrophotometric method of Benesch et al. (1973) (Shimadzu UV-160 spectrophotometer).
Haemoglobin titrations
Haemoglobin titrations were conducted according to Regan and Brauner (2010a) on concentrated stripped haemolysates that were diluted to a final concentration of 40 μmol l−1 of Hb tetramer (Hb4) and 0.1 mol l−1 KCl. A 2 ml volume of the haemolysate in the presence of GTP (guanosine 5’-triphosphate sodium salt hydrate, Sigma-Aldrich) at a molar ratio of 3:1 relative to the tetrameric Hb (GTP:Hb4) was then transferred to a chilled (12 °C), magnetically stirred glass titration vessel where the haemolysates were equilibrated with humidified oxygen (100 %) for 90 min. A 3:1 GTP:Hb4 ratio was chosen to ensure all Hb molecules came under the allosteric influence of GTP (Regan and Brauner 2010a). Although this is higher than the measured ratio of 1.63:1 found in flounder RBCs (Fletcher 1975; Val 2000), experiments by Cooper et al. (unpublished) and Pelster and Weber (1990) suggest that this difference would not affect the Hb buffer capacity or Root effect. The buffer value of GTP at this concentration was subtracted from the Hb buffer values. Hydrogen ion titrations were performed with an automated Radiometer TitraLab 90 titration apparatus (Copenhagen, Denmark), where 0.01 mol l−1 NaOH (‘Baker analysed’; J.T. Baker) was added in 10-μl increments to raise pH from iso-ionic to 9.2. After 5 min of equilibration at a pH 9.2, titration with 0.01 mol l−1 HCl (10 μl increments; ‘Baker analysed’; J.T. Baker) was initiated and continued until pH 5.2 was reached. The total amount of NaOH or HCl required to reach these endpoints was recorded. The same procedure was performed on a separate 2 ml sample from the same stock haemolysate, this time equilibrated in humidified nitrogen (100 %) to deoxygenate the Hb molecules.
The resulting titration curves were used to calculate Hb buffer values and Haldane effects. The negative slope of a titration curve at a particular pH is proportional to the Hb buffer value at that pH. Thus, buffer values between pH 5 and 9 were determined for both oxygenated and deoxygenated Hbs by calculating the negative slopes between adjacent data points on each of the oxygenated and deoxygenated Hb titration curves. Fixed acid Haldane effects were determined by calculating the vertical distances between their oxygenated and deoxygenated Hb titration curves (δZH, mol H+ taken up per mol Hb4 upon deoxygenation at constant pH).
Root effect analysis
The magnitude of the Root effect over a broad pH range was determined according to Regan and Brauner (2010b) by measuring oxygen saturation of Hb spectrophotometrically at atmospheric PO2 (157 mmHg) in Tris buffers (50 mmol l−1; Trizma hydrochloride, Sigma-Aldrich) ranging in pH from 5.5 to 8.5. Air-equilibrated concentrated haemolysates were then mixed with the buffers in a 1-ml cuvette and diluted to a final concentration of 160 mmol l−1 Hb4 and 0.1 mol l-1 KCl. This procedure was conducted for haemolysates in the presence of GTP (GTP:Hb4 ratio of 3:1). Absorption at wavelengths of 540, 560 and 576 nm were measured and recorded using a Shimadzu UV-160 spectrophotometer, and were used to calculate percent Hb-O2 saturation according to the following equations from Benesch et al. (1973):
Where A is the absorbance at either 540, 560 or 576 nm. Eq. (1) and (2) were then added together to give total Hb in solution, by which the oxygenated Hb concentration was divided to yield the percent oxygenation status of the haemolysate at each pH.
Estimating the blood acidosis within intestinal capillaries
We calculated the reduction in blood pH in the capillary of the intestine that would be expected due to intestinal HCO3 − secretion using the following assumptions for flounder in normal strength to triple strength seawater (i.e. salinities of 33 to 90):
-
1.
The non-bicarbonate buffer capacity in whole blood is proportional to the haematocrit value and can be derived from the linear regression slope of the [HCO3 −] vs. pH relationship, which has been calculated for starry flounder (Platichthys stellatus) as
where β is the buffering capacity (expressed in slykes; mmol l−1 pH−1) and Hct· is the haematocrit expressed as a fraction (Wood et al. 1982). Therefore, at haematocrits of 15–20 %, the non-bicarbonate buffer capacity would equate to approximately −5 to −6 mmol l−1 pH−1.
-
2.
The expected change in [H+] (δ [H+], mEq l−1) in the intestinal venous capillaries was calculated as:
where the potential [H+] loading rate into the blood (250–500 μEq kg−1 h−1) was divided by blood flow rate (ranging from 246 to 828 ml kg−1 h−1) (red Irish lord, Hemilepidotus hemilepidotus, Axelsson et al. 2000; European sea bass, Dicentrarchus labrax, Altimiras et al. 2008). It is important to note that intestinal blood flow rates do not exist for the species of interest. In the aforementioned studies, ultrasonic flow probes were implanted on the ventral aorta and the gastrointestinal arteries. The blood flow in the intestinal capillaries would be much lower than these, thus our estimates are extremely conservative. Potential blood [H+] loading data were taken from Whittamore et al. (2010), where Ca2+ was perfused into the intestine of flounder simulating the ingestion of seawater at salinities of 33 to 90. Incorporating the above range of blood flow rates and potential [H+] loading, a δ [H+] of between 0.3 and 2.0 mEq l−1 was predicted.
-
3.
To calculate the change in blood pH (δ pH) in the intestinal capillaries, the following equation was used:
Which accounts for the predicted H+ loading in the intestinal capillaries (δ [H+]), the non-bicarbonate buffer capacity (β), and the typical systemic difference in [HCO3 −] between venous (7.12 ± 0.32 mmol l−1; n = 5) and arterial (6.12 ± 0.37 mmol l−1; n = 4]) blood from cannulated flounder (Cooper, Whittamore and Wilson, unpublished data).
-
4.
Finally, using the following equation we converted our extracellular pH values (pHe) to red blood cell (RBC) intracellular pH (pHi):
Using constants based on data from rainbow trout at 10 °C (Heming et al. 1986).
In vivo analysis of intestinal blood acid–base balance in trout
It would be ideal to compare the above estimations of blood pH reduction within intestinal veins with those actually found in vivo in European flounder. However, in preliminary trials, it proved impossible to successfully cannulate the intestinal vein of flounder due to the complex vasculature, so we resorted to using seawater-acclimated rainbow trout as a pragmatic alternative. Seawater-acclimated rainbow trout (n = 5) were anaesthetised with MS222 (100 mg l−1 buffered with 200 mg l−1 NaHCO3, followed by prolonged aeration) and transferred to a surgery table where their gills were irrigated with temperature-controlled (14 °C) seawater containing a lower dose of buffered MS222 (60 mg l−1). The dorsal aorta was cannulated as previously described by Cooper and Wilson (2008), to provide a source of arterial blood that reflects that supplying the intestine. The ventral intestinal vein was then cannulated near the proximal end of the posterior intestine. Cannulae for the ventral intestinal vein were prepared similarly to those used for the hepatic portal vein cannulation as described by Eliason et al. (2007), with a 15-mm tip made of silastic (ID = 0.5 mm, OD = 0.94 mm) stretched over the end of PE50 tubing with a small bubble created ~3 mm from the end. A local anaesthetic (Lidocaine, 20 mg ml−1; Centaur Services, UK) was used to prepare the laparotomy site by subdermal injections (8 × 0.05 ml) along the incision line, running parallel with the lateral line from just above to slightly posterior to the right pelvic fin. A scalpel was then used to make a ~2.5 cm skin incision, and the underlying muscle was separated by scalpel and blunt dissection, and finally held open using retractors. The intestinal vein has two branches running along the dorsal and ventral sides of the intestine, connected at regular intervals by many circumferential veins that encircle the intestine (Olson, 2000). The ventral intestinal vein was located and two pieces of silk suture (4–0) were threaded between the vein and the underlying intestine about 5–8 mm apart. The posterior thread was tied to occlude the vein, and the anterior thread was loosely knotted leaving the vessel unoccluded. A small cut was then made in the vein using micro-scissors in between the two silk threads and the silastic tip of the venous cannula quickly inserted into the vein. The cannula tip was pushed forward about 15 mm into the vein and the anterior thread secured tightly around the vessel and cannula adjacent to the bubble (Eliason et al. 2007). The cannula was then flushed with a sterile solution of 150 mmol l−1 NaCl containing sodium heparin (150 I.U. ml−1). The skin incision was then closed using continuous silk sutures (2–0) and the cannula was secured to the skin at two positions, the first ~5 mm posterior to the skin incision site, and the second on the dorsal surface near the adipose fin. The skin at the incision site was then re-coated with mucus from a nearby but untreated area of skin, and the fish was recovered in anaesthetic-free seawater. Fish were closely monitored for the first 10 min during which time normal ventilation and self-righting reflexes were re-established, and then left for 24 h to recover from the surgery.
Blood samples were taken from the dorsal aorta and the ventral intestinal vein and then analysed for whole blood pH, plasma total CO2 (TCO2) and haematocrit, as described in Cooper and Wilson (2008). Plasma PCO2 and [HCO3 −] were calculated from plasma TCO2 and blood pH measurements using a rearrangement of the Henderson–Hasselbalch equation and values for solubility (αCO2 = 0.064 mmol l−1 mmHg−1) and pKapp (6.11–6.17—based on measured temperature and pH), according to Boutilier et al. (1984). An estimate of the metabolic acid addition to the blood (δH +m ) during transit from arterial to venous vessels was calculated according to McDonald et al. (1980):
where (similar to Eq. 3 for flounder), non-bicarbonate buffer values (β) were estimated from the blood haematocrit values expressed as a decimal (Hct·) using the regression relationship of Wood et al. (1982) established for rainbow trout whole blood:
Statistics
Blood acid–base variables for the paired arterial and venous sources of the same individual fish were compared using a Student’s paired t test. This included blood from the dorsal aorta and ventral intestinal vein from rainbow trout in the present study (see Table 1), as well as blood from the dorsal aorta and ventral aorta (or from an equivalent mixed venous source) from 12 previously published studies on rainbow trout (see Table 2). Means were considered significantly different when P < 0.05.
Results
Haemoglobin titrations and buffer values
Representative H+ titration curves of the oxygenated and deoxygenated Hbs from European flounder show how net proton charge (ZH, mol H+ mol−1 Hb4) of stripped Hbs in 0.1 mol l−1 KCl changes as a function of pH in the presence of GTP (3:1 molar ratio of GTP:Hb4; Fig. 1a). Zero net proton charge refers to the isoelectric pH and is used as the reference point (Tanford, 1962). Titration curves were unaffected by the different acclimation salinities.

Representative H+ titration and buffer value curves for European flounder haemoglobin. Panel A: Hb-H+ titration curves, Z H (mol H+ mol−1 Hb4) as a function of pH, for oxygenated (open symbols) and deoxygenated (filled symbols) Hb solutions. Panel B: Hb buffer values (−δZ H/δpH) as a function of pH for oxygenated (open symbols) and deoxygenated (filled symbols) Hb solutions. A total of nine titrations were performed on stripped haemolysates at a [Hb4] of 0.04 mmol l−1 and a [KCl] of 0.1 mol l−1, in the presence of organic phosphates (3:1 ratio of GTP:Hb4)
The slope of the Hb titration curve at a particular pH is representative of the Hb buffer value at that pH (mol H+ mol−1 Hb4 pH unit−1). The oxygenated Hbs of flounder exhibit a maximum buffer capacity of ~12 mol H+ mol−1 Hb4 pH unit−1 at pH 6.5, while the deoxygenated Hbs show a lower buffer value (9 mol H+ mol−1 Hb4 pH unit−1) that peaked at a higher pH (7.5; Fig. 1b). These trends are similar to the Hb-H+ binding characteristics of other teleosts measured to date.
The Haldane effect
The vertical distance, or δZH, between the oxygenated and deoxygenated titration curves indicates the fixed acid Haldane effect (δZH, mol H+ taken up per mol Hb4 upon deoxygenation at constant pH), which varies according to pH (Fig. 2). A maximum of ~3.2 H+ were taken up (by each Hb tetramer) upon deoxygenation at pH 7.0 in the presence of GTP (3:1 molar ratio of GTP:Hb4) in flounder (Fig. 2).

Fixed-acid Haldane effect (δZ H; number of protons taken up per Hb4 upon deoxygenation at constant pH) as a function of pH in European flounder, calculated from the vertical distance between the oxygenated and deoxygenated titration curves (Fig. 1)
The Root effect
Analysis of flounder Hbs revealed a significant Root effect in the presence of GTP, with an onset pH value of ~6.9 and a maximal Hb-O2 desaturation of ~55 % occurring at pH values of 6.0 and lower (Fig. 3). The Root effect properties were unaffected by the different acclimation salinities.

Root effect of European flounder haemoglobin determined spectrophotometrically in the presence of organic phosphates (3:1 ratio of GTP:Hb4). Correlation coefficient of fitted line: R 2 = 0.968
Modelling of the blood acidosis within intestinal capillaries
Our calculations (Eq. 3–6) predicted a RBC pHi reduction in the range 0.14 pH units (relatively high blood flow at the lowest salinity of 33) to 0.33 pH units (relatively low blood flow at the highest ambient salinity of 90) (Fig. 4). Assuming an arterial whole blood pH in flounder of 7.90 (Cooper et al. 2010), this would equate to an arterial pHi of 7.37. By contrast, we would predict Hbs of flounder to be exposed to pHi values from 7.37 to 7.04 in the capillaries supplying the intestinal cells when fish are living in salinities ranging from 33 to 90 (and intestinal blood flow rates ranging from 246 to 828 ml kg−1 h−1; Fig. 4).

The effects of different blood flow rates and salinities on red blood cell intracellular pH values (δpHi) in European flounder. Blood flow rates range from 246 to 828 ml kg−1 h−1, H+ loading into the blood ranges from 250 to 500 μEq kg−1 h−1, and imbibed seawater is simulated at a salinity (S) = 33(filled circles), = 60 (open circles) and = 90 (inverted triangles). See Eq. 3–6 for details
In vivo blood acid–base status of arterial and intestinal vein in seawater trout
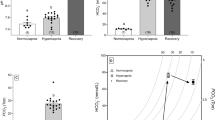
Blood from the ventral intestinal vein of seawater-acclimated trout was 0.20 pH(e) units lower on average compared to mixed arterial blood from the dorsal aorta of the same fish (Table 1). Using Eq. 6 (above), a pHe drop of 0.20 units translates to a RBC pHi decrease of 0.12 units. In contrast there was no significant difference in pH when comparing blood from mixed arterial and mixed venous sources in cannulated freshwater-acclimated rainbow trout from twelve previously published data sets (Table 2). The [HCO3 −] and PCO2 of mixed venous blood were both 25 % higher than that of mixed arterial blood (Table 2), whereas [HCO3 −] was unchanged but PCO2 was 58 % higher in the ventral intestinal vein (present study) compared to dorsal aorta (Table 1). Calculations based on Table 1 resulted in a metabolic acid load (δH +m ) of +1.9 mmol l−1 being added to the blood during transit through the vasculature of the posterior intestine of seawater trout, whereas a negative value of −1.8 mmol l−1 was calculated for δH +m when comparing mixed venous blood (either ventral aorta or Ductus of Cuvier) with the same arterial source (dorsal aorta) in freshwater-acclimated rainbow trout (Currie and Tufts 1997; Milligan and Wood 1986; Nikinmaa and Vihersaari, 1993). This represents a significantly greater net acid load of almost 4 mmol l−1 within the intestinal veins of seawater trout when compared to the average mixed venous blood.
Discussion
Through the analysis of H+ equilibria and gas exchange properties of European flounder (Platichthys flesus) Hb, we discuss how these pH-dependent Hb characteristics may be associated with enhanced O2 delivery to supply the increased metabolic demands of the intestine during the osmoregulatory work associated with drinking seawater in high salinities in marine teleosts. According to our model, osmoregulatory processes could result in intestinal capillary pHi ranging from 7.37 to 7.04 (Eqs. 3–6), placing RBC pHi directly on the “shoulder” of the Root effect curve (Fig. 3). While this means that O2 delivery may not be enhanced via the Root effect during osmoregulation in this species, this pHi change (Fig. 4) is sufficient to exploit flounder’s Bohr effect and enhance intestinal O2 delivery by up to 42 % with no change to tissue blood flow (Fig. 5). While this phenomenon has yet to be quantified directly in vivo, it is likely applicable to all teleost fish in hyperosmotic environments.

Oxygen equilibrium curves (OECs) for European flounder haemoglobin modelled using the Hill equation. Solid curve represents resting red blood cell (RBC) pHi of 7.37 and is based on a Hb P50 value of 30 mmHg (Jensen et al. 2002) and a Hill coefficient of 1.2 (Jensen et al. 2002), while hashed curves represent those OECs at RBC pHi values below resting levels. Filled circles enclosed in box depict differences in Hb-O2 at a PO2 approximating venous levels (40 mmHg, based on Cooper et al. 2010) as a function of pHi, with lower case letters showing differences in Hb-O2 saturation that come with a, a 0.1, b 0.2, c 0.3 and d 0.4 reduction in RBC pHi below resting levels. Bolded “a” at top of figure represents arterial Hb-O2 saturation percentage of 100 %, while bolded “v” represents venous Hb-O2 saturation percentage of 58 % (based on the aforementioned 40 mmHg venous PO2). Filled squares represent the PO2 changes that result from a 0.1 and 0.2 reduction in RBC pHi at a constant Hb-O2 saturation percentage of 58 % (see discussion for details)
The potential for enhanced O2 delivery to the intestinal cells via the Bohr effect
The degree to which O2 delivery to intestinal cells could be enhanced is a product of the RBC pHi change during blood capillary transit and the intracellular Bohr coefficient. While the Haldane effect describes the change in Hb-H+ affinity that results from a change in Hb-O2 saturation, the Bohr effect describes a change in Hb-O2 affinity that results from a change in pH. These two phenomena are thermodynamically linked at the molecular level (Wyman, 1973), and this linkage is illustrated by the equation:
where δH+ is the number of moles of protons released per mole of O2 bound to Hb (i.e. the Haldane coefficient, derived from Fig. 2), and the Bohr coefficient is the numerical negative of this value (Jensen and Weber, 1985). At a pHi of 7.37, the Hb of European flounder releases 2.52 mol of protons for every 4 mol of O2 bound, resulting in a Haldane coefficient of 0.63 and thus a Bohr coefficient of −0.63. Assuming a blood P 50 (PO2 at which Hb is 50 % saturated) value of 30 mmHg (Jensen et al. 2002), changes in P 50 can be estimated over the calculated range of RBC pHi values within intestinal capillaries determined at the respective salinity and intestinal blood flow rates given above (Eq. 3–6; Fig. 4). Oxygen equilibrium curves (OECs) can then be constructed from these δP 50 values by re-arranging the Hill equation (Hill, 1910):
where y is Hb-O2 saturation and n is the Hill coefficient of European flounder (1.2, from Jensen et al. 2002). The resulting curves are depicted in Fig. 5, where the solid line represents the OEC at control values for RBC pHi, and the four hashed lines beneath it represent calculated OECs at progressively lower RBC pHi values.
The degree to which the calculated RBC pHi changes could enhance O2 delivery can be interpolated directly from these OECs. Assuming that arterial blood saturation is always close to 100 % and venous PO2 (P vO2) is 40 mmHg (Cooper et al. 2010), the a-v Hb-O2 extraction with no change in RBC pHi (Fig. 5 solid line) would be 42 % (i.e. 100 − 58 %). The calculated reductions in RBC pHi result in a large increase in P vO2 with constant a-v Hb-O2 extraction (i.e. trace horizontally across the curves from the point mentioned above), increasing the driving force for O2 delivery. For example, P vO2 would be increased from 40 mmHg to 46 or 53.5 mmHg with a 0.1 or 0.2 pHi unit reduction, respectively. Assuming a constant P vO2 (whereby enhanced metabolism by the tissues instantly draws the “extra” O2 available from the blood), the calculated reductions in RBC pHi could have a large effect on a-v Hb-O2 saturation, thus enhancing delivery. Again assuming arterial saturation remains close to 100 %, a drop in RBC pHi of 0.1 units would increase a-v Hb-O2 extraction to 45 % (point a, Fig 5; 100 − 55 %), which could represent a 7 % increase in O2 delivery relative to the control (45/42 × 100 = 107 %) with no change in blood flow or P vO2. A similar analysis for a RBC pHi reductions of 0.2, 0.3 and 0.4 units yields an enhanced O2 delivery relative to the control of 20 % (point b, Fig 5; 50.5/42 × 100 = 120 %), 31 % (point c, Fig 5; 55/42 × 100 = 131 %) and 42 % (point d, Fig 5; 59.5/42 × 100 = 142 %), respectively, indicating that this system has a tremendous potential to facilitate O2 delivery to this metabolically active tissue.
The RBC pHi reductions discussed above were calculated instead of being measured because the cannulation of flounder’s intestinal vein proved impossible and, to our knowledge, no other direct measurements from the intestinal capillaries of flounder or any other species have been made. However, we were able to successfully cannulate the ventral intestinal vein of seawater-acclimated rainbow trout. In vivo pHe measurements were consistently 0.2 pH units lower than mixed arterial blood from the dorsal aorta (Table 1), equating to a pHi decrease of 0.12 pH units (Eq. 6). This difference in blood pH is likely directly associated with osmoregulation in a marine environment, as the pH differences between mixed arterial and mixed venous sources of blood are minimal or in some cases even reversed (Brauner et al. 2000a, b; and see Table 2). These in vivo measurements match the predictions made by our model, when using trout-specific data, remarkably well. For example, when using a non-bicarbonate buffer (β) value of −9.48 calculated for rainbow trout whole blood (Wood et al. 1982) and measured values for arterial pHe (7.93; Table 1), arterial and venous HCO3 − concentration (11.40 mmol l−1; Table 1), and H+ loading into the venous blood (1.9 mmol l−1; dorsal aorta vs. ventral intestinal vein), the pHi prediction of our rainbow trout model is consistent with the measured values (i.e. a reduction of 0.12 pHi units; Eq. 5 and 6). Taking these calculations forward, again using trout-specific data, trout OECs can be produced and then compared to those from flounder. Using an intracellular trout Bohr coefficient of −0.70 (Jensen, 1989), a P 50 value of 23 mmHg (Tetens and Christensen, 1987), a P vO2 of 55 mmHg (Brauner et al. 2000a), and assuming that arterial blood saturation is always close to 100 %, our trout OECs predict that a drop in RBC pHi of 0.1 units would represent a 18 % increase in O2 delivery relative to the control (Eq. 10). This is similar to what was calculated in the flounder model (i.e. a 0.1 pHi decrease equating to a 7 % increase in O2 delivery relative to the control; Fig. 5). It is worth noting that predictions for a pHi decrease of 0.1 units in both species are based on these fish osmoregulating in normal strength seawater. Our flounder model goes a step further and uses H+ loading data from fish osmoregulating in double and triple strength seawater. Although extreme, this model demonstrates the potential for osmoregulation in hyperosmotic environments to directly enhance O2 delivery to the enterocytes.
The measured pH reduction in vivo is physiologically significant and very close to our calculated predicted change in blood pH. Importantly, these predictions are likely an underestimate of the most extreme potential pH change occurring in the blood supplying HCO3 −-secreting enterocytes for two reasons. Firstly, the intestinal vein we cannulated collects venous blood that drains from all the tissues of the intestine, the major volume of which will be the submucosa, and the circular and longitudinal smooth muscle layers, whereas the HCO3 −-secreting epithelium adjacent to the gut lumen will make up the minor portion. Secondly, the highest rates of intestinal HCO3 − secretion are likely to be from those cells located in the anterior region, where the ingested Ca2+ ions that drive HCO3 − secretion first enter the intestine (Wilson et al. 2002). By contrast, we cannulated the ventral intestinal vein at the posterior end of the intestine. Attempts were made to directly access the venous blood draining the anterior section of the intestine, but this proved to be impossible due to the location of the pyloric caeca in rainbow trout. Nevertheless, this conservative measurement of the arterial–venous blood pH difference is still very large (Fig. 5), and one that is certainly capable of increasing the O2 delivery potential of H+ sensitive Hbs.
This level of enhanced O2 delivery may be important to satisfy the metabolic demands of intestinal tissue. European flounder acclimated to double strength seawater (salinity = 60) were shown to have a 50 % higher O2 consumption rate at the whole body level than those acclimated to a salinity of 33 (2.25 vs. 1.5 mmol kg−1 h−1; Cooper and Wilson, unpublished). It is not known whether these whole body metabolic changes are representative of those that would occur at the intestinal epithelium, however, using isolated intestinal tissue in a specialized in vitro Ussing chamber set-up, Taylor and Grosell (2009) showed that following a meal, O2 consumption and HCO3 − secretion increased 1.9- and 1.6-fold, respectively. These data highlight how metabolically demanding HCO3 − secretion can be, both in vivo and in vitro. Any increase in intestinal PO2 initiated by the Bohr effect would therefore be of major benefit to the fish.
Finally, it is also relevant to note that the total CO2 (11.70 ± 1.04 mmol l−1) in the intestinal vein of rainbow trout was not significantly different from that in the arterial supply (11.54 ± 0.73 mmol l−1) to this tissue (reflected in the data for plasma [HCO3 −] in Table 1), whereas mixed venous blood typically has a total CO2 (and [HCO3 −]) that is 2 mmol l−1 or about 25 % higher than mixed arterial blood (Table 2). This suggests there was zero net excretion of respiratory CO2 from the intestine into the blood. Taken at face value, this suggests that the demand for apical HCO3 − secretion was equivalent to the entire respiratory CO2/HCO3 − produced by all the tissues supplied by the intestinal vasculature (i.e. the epithelium plus underlying submucosa, and circular and longitudinal smooth muscle layers etc.). It therefore seems likely that apical HCO3 − secretion by the enterocytes cannot be fuelled by their endogenous respiratory CO2 production alone, even under the relatively mild hyperosmotic conditions of normal seawater. This situation will be even more extreme under hypersaline conditions—the intestine is likely to become a net consumer of both CO2 and O2 from its vascular blood supply, rather than driving a roughly equal exchange of these two respiratory gases as is the norm in animal tissues.
Additional mechanisms for enhanced O2 delivery to the intestine
The teleost eye and swim bladder have long been posited as the only tissues in the body capable of generating sufficient blood acidoses to activate the Root effect and greatly enhance oxygen delivery. But recent work suggests that a mild acidosis in the presence of plasma-accessible carbonic anhydrase (CA) may greatly enhance oxygen delivery in muscle too. In a closed in vitro system, the addition of plasma-accessible CA to acidified rainbow trout RBCs has been shown to short circuit pH regulation via Na+/H+ exchange (NHE), decreasing Hb-O2 saturation and elevating blood PO2 by ~30 mmHg (Rummer and Brauner, 2011). In vivo, plasma-accessible CA in the presence of a mild acidosis has been estimated to double muscle oxygen delivery with no change in blood flow (Rummer et al. 2013). Our model for the intestine does not take into account the potential effect of plasma-accessible CA on RBC pHi. However, in the enterocytes of teleost fishes, various CA isoforms are present on the apical membrane and in the cytosol (Gilmour et al. 2012; Grosell et al. 2007; Sattin et al. 2010) similar to the muscle (Wang et al. 1998; Henry and Swenson, 2000) and the arterial blood supply (Randall et al. 2014), and potentially in the basolateral extracellular fluid (although this has yet to be characterized, Taylor et al. 2011). It is therefore likely that RBCs in close proximity to the intestine will come into contact with CA. Exposing the intestine to hypersaline conditions results in a mild systemic-wide blood acidosis (Cooper et al. 2010), which in the presence of plasma-accessible CA, could be transmitted to the RBC, further reducing pHi from those calculated here. If operational, our pHi calculations could be a considerable underestimation, and O2 delivery may be enhanced to an even greater degree than that proposed here owing to a potential Root effect-activating blood acidosis (i.e. pH 6.9; Fig. 3). Further studies at the capillary level will be necessary to elucidate the role of plasma-accessible CA in maximizing O2 delivery to the intestinal cells. Plasma-accessible CA could also hasten the RBC acidosis, which could be important if capillary transit times through the intestine are very short. We are currently pursuing further studies at the capillary level to determine transit times, confirm the presence of plasma-accessible CA at the intestine and to evaluate its potentially crucial role in maximizing O2 delivery to the intestinal cells.
Concluding remarks
We have shown that the marine teleost intestine may take advantage of the unique pH-dependent properties of teleost Hb to greatly enhance O2 delivery to the intestinal cells that have constitutively high-energy demands associated with their osmoregulatory role in hyperosmotic environments. It was hypothesized that the secretion of HCO3 − into the intestinal lumen that results in an equivalent transfer of protons into the blood supply would decrease RBC pHi sufficiently to exploit the Bohr and possibly Root effects, enhancing O2 delivery. Our analysis of European flounder Hb properties allowed us to construct a model that suggests this is indeed the case. Furthermore, when trout-specific values were used for the model’s variables, the resulting predictions are consistent with the measured in vivo pH difference between arterial and venous blood serving the intestine of seawater-acclimated rainbow trout, lending further support to the model. An extremely conservative estimate suggests a 0.1 unit pH change in the intestinal blood supply would enhance O2 delivery to enterocytes by 7 %. A more realistic estimation of intestinal blood pH change suggests this number is no less than 25 % in fish at normal marine salinities. If plasma-accessible carbonic anhydrase is present at the intestinal cell, then RBC pHi could be even further reduced, with correspondingly greater increases in O2 delivery. To accurately confirm this, micro-scale pH measurements within intestinal capillaries are required, and thus warrants further investigation.
Intriguingly, the system we propose would serve as an elegant example of autoregulation linking osmoregulation and gas transport to satisfy the energetic costs of hypo-osmoregulation in teleosts. In essence, the greater the demand for metabolically sourced HCO3 − resulting from increased salinity and drinking rate, the greater the enhancement of O2 delivery to the intestine via a localized acidosis and a pH-sensitive Hb. This would operate in all marine teleosts, but such autoregulation may be especially important for fish living in variable salinity environments, and in particular, hypersaline environments. A suitable species with respect to the “Krogh Principle” for studying this phenomenon would be the Arabian killifish (Aphanius dispar), a remarkable animal capable of living in salinities five times greater than seawater (Plaut, 2000). In any case, our results suggest that the marine teleost intestine may utilize a pH-dependent mechanism of enhanced O2 delivery. This autoregulation would specifically support the osmoregulatory component of this truly multifunctional organ in fish, adding to the intrigue of its various roles in digestion, nutrient absorption, excretion, acid–base regulation and gas exchange.
References
Altimiras J, Claireaux G, Sandblom E, Farrell AP, McKenzie DJ, Axelsson M (2008) Gastrointestinal blood flow and postprandial metabolism in swimming sea bass Dicentrarchus labrax. Physiol Biochem Zool 81(5):663–672
Aschauer H, Weber RE, Braunitzer G (1985) The primary structure of the hemoglobin of the dogfish shark (Squalus acanthias) Antagonistic effects of ATP and urea on oxygen affinity of an elasmobranch hemoglobin. Biol Chem Hoppe Seyler 366(6):589–599
Axelsson M, Thorarensen H, Nilsson S, Farrell AP (2000) Gastrointestinal blood flow in the red Irish lord, Hemilepidotus hemilepidotus: long-term effects of feeding and adrenergic control. J Comp Physiol B 170(2):145–152
Benesch RE, Benesch R, Yung S (1973) Equations for the spectrophotometric analysis of hemoglobin mixtures. Anal Biochem 55(1):245–248
Berenbrink M (2006) Evolution of vertebrate haemoglobins: histidine side chains, specific buffer value and Bohr effect. Respir Physiol Neurobiol 154:165–184
Berenbrink M, Koldkjaer P, Kepp O, Cossins AR (2005) Evolution of oxygen secretion in fishes and the emergence of a complex physiological system. Science 307:1752–1757
Boutilier RG, Heming TA, Iwama GK (1984) Appendix: physicochemical parameters for use in fish respiratory physiology. Fish Physiol 10:403–430
Brauner CJ, Randall DJ (1996) The interaction between oxygen and carbon dioxide movements in fishes. Comp Biochem Physiol A 113(1):83–90
Brauner CJ, Weber RE (1998) Hydrogen ion titrations of the anodic and cathodic haemoglobin components of the European eel, Anguilla Anguilla. J Exp Biol 201:2507–2514
Brauner CJ, Thorarensen H, Gallaugher P, Farrell AP, Randall DJ (2000a) CO2 transport and excretion in rainbow trout (Oncorhynchus mykiss) during graded sustained exercise. Respir Physiol 119(1):69–82
Brauner CJ, Thorarensen H, Gallaugher P, Farrell AP, Randall DJ (2000b) The interaction between O2 and CO2 in the blood of rainbow trout (Oncorhynchus mykiss) during graded sustained exercise. Respir Physiol 119(1):83–96
Braunitzer G, Gehring-Mueller R, Hilschmann N, Hilse K, Hobom G, Rudloff V, Wittmann-Liebold B (1961) The structure of normal adult human haemoglobins. Hoppe Seylers Z Physiol Chem 325:283–286
Cameron JN, Heisler N (1983) Studies of ammonia in the rainbow trout: physicochemical parameters, acid–base behaviour and respiratory clearance. J Exp Biol 105:107–125
Cooper CA, Wilson RW (2008) Post-prandial alkaline tide in freshwater rainbow trout: effects of meal anticipation on recovery from acid–base and ion regulatory disturbances. J Exp Biol 211:2542–2550
Cooper CA, Whittamore JM, Wilson RW (2010) Ca2+-driven intestinal HCO -3 secretion and CaCO3 precipitation in the European flounder in vivo: influences on acid–base regulation and blood gas transport. Am J Physiol Regul Integr Comp Physiol 298:870–876
Currie S, Tufts BL (1997) Synthesis of stress protein 70 (hsp 70) in rainbow trout red blood cells. J Exp Biol 200:607–614
Drabkin DL, Austin JH (1935) Spectrophotometric studies Preparations from washed blood cells; nitric oxide hemoglobin and sulfhemoglobin. J Biol Chem 112:51–65
Eliason EJ, Kiessling A, Karlsson A, Djordjevic B, Farrell AP (2007) Validation of the hepatic portal vein cannulation technique using Atlantic salmon Salmo salar L. J Fish Biol 71:290–297
Fletcher GL (1975) The effects of capture, “stress,” and storage of whole blood on the red blood cells, plasma proteins, glucose, and electrolytes of the winter flounder (Pseudopleuronectes americanus). Can J Zool 53:197–206
Genz J, Taylor JR, Grosell M (2008) Effects of salinity on intestinal bicarbonate secretion and compensatory regulation of acid–base balance in Opsanus beta. J Exp Biol 211:2327–2335
Gilmour KM, Perry SF, Esbaugh AJ, Genz J, Taylor JR, Grosell M (2012) Compensatory regulation of acid–base balance during salinity transfer in rainbow trout (Oncorhynchus mykiss). J Comp Physiol B 182(2):259–274
Grosell M (2006) Intestinal anion exchange in marine fish osmoregulation. J Exp Biol 209:2813–2827
Grosell M (2010) The role of the gastrointestinal tract in salt and water balance. Fish Physiol 30:135–164
Grosell M (2011) Intestinal anion exchange in marine teleosts is involved in osmoregulation and contributes to the oceanic inorganic carbon cycle. Acta Physiol 202(3):421–434
Grosell M, Genz J (2006) Ouabain-sensitive bicarbonate secretion and acid absorption by the marine teleost fish intestine play a role in osmoregulation. Am J Physiol Regul Integr Comp Physiol 291:1145–1156
Grosell M, Wood CM, Wilson RW, Bury NR, Hogstrand C, Rankin C, Jensen FB (2005) Bicarbonate secretion plays a role in chloride and water absorption of the European flounder intestine. Am J Physiol Regul Integr Comp Physiol 288:936–946
Grosell M, Gilmour KM, Perry SF (2007) Intestinal carbonic anhydrase, bicarbonate, and proton carriers play a role in the acclimation of rainbow trout to seawater. Am J Physiol Regul Integr Comp Physiol 293(5):2099–2111
Grosell M, Genz J, Taylor JR, Perry SF, Gilmour KM (2009a) The involvement of H+-ATPase and carbonic anhydrase in intestinal HCO -3 secretion on seawater-acclimated rainbow trout. J Exp Biol 212:1940–1948
Grosell M, Mager EM, Williams C, Taylor JR (2009b) High rates of HCO3- secretion and Cl– absorption against adverse gradients in the marine teleost intestine: the involvement of an electrogenic anion exchanger and H+- pump metabolon? J Exp Biol 212:1684–1696
Heming TA, Randall DJ, Boutilier RG, Iwama GK, Primmett D (1986) Ionic equilibria in red blood cells of rainbow trout (Salmo gairdneri): Cl-, HCO -3 and H+. Respir Physiol 65(2):223–234
Henry RP, Swenson ER (2000) The distribution and physiological significance of carbonic anhydrase in vertebrate gas exchange organs. Respir Physiol 121:1–12
Hill AV (1910) The possible effects of the aggregation of the molecules of haemoglobin on its dissociation curves. J Physiol 40:4–7
Holeton GF, Randall DJ (1967) The effect of hypoxia upon the partial pressure of gases in the blood and water afferent and efferent to the gills of rainbow trout. J Exp Biol 46(2):317–327
Jensen FB (1989) Hydrogen ion equilibria in fish haemoglobins. J Exp Biol 143:225–234
Jensen FB (2001) Hydrogen ion binding properties of tuna haemoglobins. Comp Biochem Physiol A 129:511–517
Jensen FB, Weber RE (1985) Proton and oxygen equilibria, their anion sensitivities and interrelationships in tench hemoglobin. Mol Physiol 7:41–50
Jensen FB, Fago A, Weber RE (1998) Red blood cell physiology and biochemistry. Fish Physiol Fish Respir 17:1–40
Jensen FB, Lecklin T, Busk M, Bury NR, Wilson RW, Wood CM, Grosell M (2002) Physiological impact of salinity increase at organism and red blood cell levels in the European flounder (Platichthys flesus). J Exp Mar Biol Ecol 274:159–174
Kiceniuk JW, Jones DR (1977) The oxygen transport system in trout (Salmo gairdneri) during exercise. J Exp Biol 69:247–260
Lapennas GN (1983) The magnitude of the Bohr coefficient: optimal for oxygen delivery. Respir Physiol 54(2):161–172
McDonald DG, Hobe H, Wood CM (1980) The influence of calcium on the physiological responses of the rainbow trout, Salmo gairdneri, to low environmental pH. J Exp Biol 88:109–131
Milligan CL, Wood CM (1986) Intracellular and extracellular acid–base status and H+ exchange with the environment after exhaustive exercise in the rainbow trout. J Exp Biol 123:93–121
Nikinmaa M, Vihersaari L (1993) Pre- and postbranchial carbon dioxide content of rainbow trout (Oncorhynchus mykiss) blood after catecholamine injection. J Exp Biol 180:315–321
Olson KR (2000) Circulatory system. The laboratory fish K O Gary. Academic Press, London, pp 161–171
Pelster B, Randall DJ (1998) The physiology of the Root effect. Fish Physiol Fish Respir 17:113–140
Pelster B, Weber RE (1990) Influence of organic phosphates on the Root effect of multiple fish haemoglobins. J Exp Biol 149:425–437
Perry SF, Brauner CJ, Tufts B, Gilmour KM (1997) Acid–base disequilibrium in the venous blood of rainbow trout (Oncorhynchus mykiss). Exp Biol Online 2(1):1–10
Perry SF, Rivero-Lopez L, McNeill B, Wilson J (2006) Fooling a freshwater fish: how dietary salt transforms the rainbow trout gill into a seawater gill phenotype. J Exp Biol 209:4591–4596
Plaut I (2000) Resting metabolic rate, critical swimming speed, and routine activity of the euryhaline cyprinodontid, Aphanius dispar, acclimated to a wide range of salinities. Physiol Biochem Zool 73(5):590–596
Randall DJ, Brauner C (1998) Interactions between ion and gas transfer in freshwater teleost fish. Comp Biochem Physiol A 119(1):3–8
Randall DJ, Rummer JL, Wilson JM, Wang S, Brauner CJ (2014) Oxygen delivery to tissues and the radiation of teleost fish. J Exp Biol 217:1205–1214
Regan M, Brauner CJ (2010a) The transition in haemoglobin proton-binding characteristics within the basal actinopterygian fishes. J Comp Physiol B 180:521–530
Regan M, Brauner CJ (2010b) The evolution of Root effect haemoglobins in the absence of intracellular pH protection of the red blood cell: insights from primitive fishes. J Comp Physiol B 180:695–706
Root RW (1931) The respiratory function of the blood of marine fishes. Biol Bull 61:427–456
Root RW, Irving L (1943) The effect of carbon dioxide and lactic acid on the oxygen combining power of whole and hemolysed blood of the marine fish Tautogaonitis (Linn). Biol Bull Mar Biol Lab Woods Hole 84:207–212
Rummer JL, Brauner CJ (2011) Plasma-accessible carbonic anhydrase at the tissue of a teleost fish may greatly enhance oxygen delivery: in vitro evidence in rainbow trout (Oncorhynchus mykiss). J Exp Biol 214:2319–2328
Rummer JL, McKenzie DJ, Innocenti A, Supuran CT, Brauner CJ (2013) Root effect hemoglobin may have evolved to enhance general tissue oxygen delivery. Science 340(6138):1327–1329
Salman NA, Eddy FB (1990) Increased sea-water adaptability of non-smolting rainbow trout by salt feeding. Aquacult 86(2–3):259–270
Sattin G, Mager EM, Beltramini M, Grosell M (2010) Cytosolic carbonic anhydrase in the Gulf toadfish is important for tolerance to hypersalinity. Comp Biochem Physiol A 156(2):169–175
Soivio A, Nikinmaa M, Nyholm K, Westman K (1981) The role of gills in the responses of Salmo gairdneri to moderate hypoxia. Comp Biochem Physiol A 70:133–139
Tanford C (1962) The interpretation of hydrogen ion titration curves of proteins. Adv Protein Chem 17:69–165
Taylor JR, Grosell M (2009) The intestinal response to feeding in seawater gulf toadfish, Opsanus beta, includes elevated base secretion and increased epithelial oxygen consumption. J Exp Biol 212(23):3873–3881
Taylor JR, Cooper CA, Mommsen TP (2011) Implications of GI function for gas exchange, acid–base balance and nitrogen metabolism. Fish Physiol 30:213–260
Tetens V, Christensen NJ (1987) β-Adrenergic control of blood oxygen affinity in acutely hypoxia exposed rainbow trout. J Comp Physiol B 157:667–675
Thomas S, Fritsche R, Perry SF (1994) Pre- and post-brachial blood respiratory status during acute hypercapnia or hypoxia in rainbow trout, Oncorhynchus mykiss. J Comp Physiol B 164:451–458
Val AL (2000) Organic phosphates in the red blood cells of fish. Comp Biochem Physiol A 125(4):417–435
Walsh PJ, Blackwelder P, Gill KA, Danulat E, Mommsen TP (1991) Carbonate deposits in marine fish intestines–a new source of biomineralisation. Limnol Oceanogr 38:1227–1232
Wang Y, Henry RP, Wright PM, Heigenhauser GJF, Wood CM (1998) Respiratory and metabolic functions of carbonic anhydrase in exercised white muscle of trout. Am J Physiol Regul Integr Comp Physiol 275:R1766–R1779
Whittamore JM, Cooper CA, Wilson RW (2010) HCO -3 secretion and CaCO3 precipitation play major roles in intestinal water absorption in marine teleost fish in vivo. Am J Physiol Regul Integr Comp Physiol 298(4):877–886
Wilson RW, Grosell M (2003) Intestinal bicarbonate secretion in marine teleost fish–source of bicarbonate, pH sensitivity, and consequences for whole animal acid–base and calcium homeostasis. Biochim Biophys Acta 1618:163–174
Wilson RW, Wilson JM, Grosell M (2002) Intestinal bicarbonate secretion by marine teleost fish-why and how? Biochim Biophys Acta 1566:182–193
Wolf K (1963) Physiological salines for freshwater teleosts. Prog Fish Cult 25:135–140
Wood CM (1991) Acid–base and ion balance, metabolism and their interactions, after exhaustive exercise in fish. J Exp Biol 160:285-08
Wood CM, McDonald DG, McMahon BR (1982) The influence of experimental anaemia on blood acid–base regulation in vivo and in vitro in the starry flounder (Platichthys stellatus) and the rainbow trout (Salmo gairdneri). J Exp Biol 96:221–237
Wyman J (1973) Linked functions and reciprocal effects in haemoglobin: A second look. Adv Protein Chem 16:223–286
Acknowledgments
Underlying research materials, i.e. raw data, is accessible by contacting the corresponding author, Dr. Rod Wilson at r.w.wilson@ex.ac.uk. This research was supported by BBSRC and NERC grants (BB/D005108/1 and NE/H010041/1) to RWW and an NSERC Discovery grant to CJB. We would like to thank Jan Shears for excellent technical support and fish husbandry.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Communicated by I.D. Hume.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article

Cite this article
Cooper, C.A., Regan, M.D., Brauner, C.J. et al. Osmoregulatory bicarbonate secretion exploits H+-sensitive haemoglobins to autoregulate intestinal O2 delivery in euryhaline teleosts. J Comp Physiol B 184, 865–876 (2014). https://doi.org/10.1007/s00360-014-0844-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00360-014-0844-x