
Abstract
Purpose
To evaluate urinary continence (UC) recovery and oncological outcomes in different risk-groups after robot-assisted radical prostatectomy (RALP) and open retropubic radical prostatectomy (RRP).
Patients and methods
We analysed 2650 men with prostate cancer from seven open (n = 805) and seven robotic (n = 1845) Swedish centres between 2008 and 2011 in a prospective non-randomised trial, LAPPRO. UC recovery was defined as change of pads less than once in 24 h. Information was collected through validated questionnaires. Rate of positive surgical margins (PSM) and biochemical recurrence (BCR), defined as prostate-specific antigen (PSA) > 0.25 mg/ml, were recorded. We stratified patients into two risk groups (low-intermediate and high risk) based on the D’Amico risk classification system.
Result
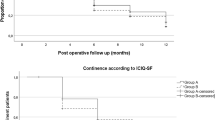
Among men with high-risk prostate cancer, we found significantly higher rates of UC recovery up to 24 months after RRP compared to RALP (66.1% vs 60.5%) RR 0.85 (CI 95% 0.73–0.99) while PSM was more frequent after RRP compared to RALP (46.8% vs 23.5%) RR 1.56 (CI 95% 1.10–2.21). In the same group no significant difference was seen in BCR. Overall, however, BCR was significantly more common after RRP compared to RALP at 24 months (9.8% vs 6.6%) RR 1.43 (Cl 95% 1.08–1.89). The limitations of this study are its non-randomized design and the relatively short time of follow-up.
Conclusions
Our study indicates that men with high-risk tumour operated with open surgery had better urinary continence recovery but with a higher risk of PSM than after robotic-assisted laparoscopic surgery. No significant difference was seen in biochemical recurrence.
Trial registration
ISRCTN06393679.

Similar content being viewed by others


Data availability
This manuscript has associated data which will not be deposited.
References
Sooriakumaran P, Ploumidis A, Nyberg T, Olsson M, Akre O, Haendler L et al (2015) The impact of length and location of positive margins in predicting biochemical recurrence after robot-assisted radical prostatectomy with a minimum follow-up of 5 years. BJU Int 115(1):106–113
Sooriakumaran P, Pini G, Nyberg T, Derogar M, Carlsson S, Stranne J et al (2018) Erectile function and oncologic outcomes following open retropubic and robot-assisted radical prostatectomy: results from the LAParoscopic prostatectomy robot open trial. Eur Urol 73(4):618–627
Ficarra V, Novara G, Rosen RC, Artibani W, Carroll PR, Costello A et al (2012) Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy. Eur Urol 62(3):405–417
Wallerstedt A, Tyritzis SI, Thorsteinsdottir T, Carlsson S, Stranne J, Gustafsson O et al (2015) Short-term results after robot-assisted laparoscopic radical prostatectomy compared to open radical prostatectomy. Eur Urol 67(4):660–670
Patel VR, Schatloff O, Chauhan S, Sivaraman A, Valero R, Coelho RF et al (2012) The role of the prostatic vasculature as a landmark for nerve sparing during robot-assisted radical prostatectomy. Eur Urol 61(3):571–576
Haglind E, Carlsson S, Stranne J, Wallerstedt A, Wilderang U, Thorsteinsdottir T et al (2015) Urinary incontinence and erectile dysfunction after robotic versus open radical prostatectomy: a prospective, controlled. Nonrandomised Trial Eur Urol 68(2):216–225
Nyberg M, Hugosson J, Wiklund P, Sjoberg D, Wildera U, Carlsson S, Carlsson S, Stranne J, Steineck G, Haglind E, Bjartell A (2018) Functional and oncologic outcomes between open and robotic radical prostatectomy at 24-month follow-up in the Swedish LAPPRO trial. Eur Urol Oncol 1:353–360
Thorsteinsdottir T, Stranne J, Carlsson S, Anderberg B, Bjorholt I, Damber JE et al (2011) LAPPRO: a prospective multicentre comparative study of robot-assisted laparoscopic and retropubic radical prostatectomy for prostate cancer. Scand J Urol Nephrol 45(2):102–112
Steineck G, Hunt H, Adolfsson J (2006) A hierarchical step-model for causation of bias-evaluating cancer treatment with epidemiological methods. Acta Oncol 45(4):421–429
Steineck G, Bergmark K, Henningsohn L, Abany M, Dickman PW, Helgason A (2002) Symptom documentation in cancer survivors as a basis for therapy modifications. Acta Oncol. 41(3):244–252
D’Amico AV, Whittington R, Malkowicz SB, Schultz D, Blank K, Broderick GA et al (1998) Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 280(11):969–974
Persson J, Wilderang U, Jiborn T, Wiklund PN, Damber JE, Hugosson J et al (2014) Interobserver variability in the pathological assessment of radical prostatectomy specimens: findings of the Laparoscopic Prostatectomy Robot Open (LAPPRO) study. Scand J Urol 48(2):160–167
Xu S, Ross C, Raebel MA, Shetterly S, Blanchette C, Smith D (2010) Use of stabilized inverse propensity scores as weights to directly estimate relative risk and its confidence intervals. Value Health 13(2):273–277
White IR, Royston P, Wood AM (2011) Multiple imputation using chained equations: Issues and guidance for practice. Stat Med 30(4):377–399
Little RJ, D’Agostino R, Cohen ML, Dickersin K, Emerson SS, Farrar JT et al (2012) The prevention and treatment of missing data in clinical trials. N Engl J Med 367(14):1355–1360
Mitra R, Reiter JP (2016) A comparison of two methods of estimating propensity scores after multiple imputation. Stat Methods Med Res 25(1):188–204
Coughlin GD, Yaxley JW, Chambers SK, Occhipinti S, Samaratunga H, Zajdlewicz L et al (2018) Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: 24-month outcomes from a randomised controlled study. Lancet Oncol 19(8):1051–1060
Abdollah F, Dalela D, Sood A, Sammon J, Cho R, Nocera L et al (2017) Functional outcomes of clinically high-risk prostate cancer patients treated with robot-assisted radical prostatectomy: a multi-institutional analysis. Prostate Cancer Prostatic Dis 20(4):395–400
Novara G, Ficarra V, Mocellin S, Ahlering TE, Carroll PR, Graefen M et al (2012) Systematic review and meta-analysis of studies reporting oncologic outcome after robot-assisted radical prostatectomy. Eur Urol 62(3):382–404
Rajan P, Hagman A, Sooriakumaran P, Nyberg T, Wallerstedt A, Adding C, et al. Oncologic Outcomes After Robot-assisted Radical Prostatectomy: A Large European Single-centre Cohort with Median 10-Year Follow-up. Eur Urol Focus. 2016.
Sooriakumaran P, Srivastava A, Shariat SF, Stricker PD, Ahlering T, Eden CG et al (2014) A multinational, multi-institutional study comparing positive surgical margin rates among 22393 open, laparoscopic, and robot-assisted radical prostatectomy patients. Eur Urol 66(3):450–456
Ritch CR, You C, May AT, Herrell SD, Clark PE, Penson DF et al (2014) Biochemical recurrence-free survival after robotic-assisted laparoscopic vs open radical prostatectomy for intermediate- and high-risk prostate cancer. Urology 83(6):1309–1315
Acknowledgements
The study was supported by research grants from the Swedish Research Council (2012-1770, 2015-02483), the Swedish Cancer Society (2010/503, 2013/497, 2016/362), Region Västra Götaland, Sahlgrenska University Hospital (ALF Grants 138751, 4307771, 718221 agreement concerning research and education of doctors), Mrs. Mary von Sydow Foundation, Anna and Edvin Berger Foundation. Dr Anna Lantz was supported by research Grants from the Stockholm County Council (20170579) and Swedish Medical Association (SLS-882441).
Funding
Peter Wiklund certifies that all conflicts of interest, including specific financial interests and relationships and affiliations relevant to the subject matter or materials discussed in the manuscript (eg, employment/affiliation, grants or funding, consultancies, honoraria, stock ownership or options, expert testimony, royalties, or patents filed, received, or pending), are the following: None.
Author information
Authors and Affiliations
Contributions
NPW had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: AH, AL, GS, NPW, EH. Acquisition of data: EH, AB, Carlsson, Wiklund, Steineck, Hugosson, Stranne. Analysis and interpretation of data: AH, PW, OA, AL, GS, SC, JH, JS, SIT, EH, AB, JH. Drafting of the manuscript: AH, AL, PW, OA. Critical revision of the manuscript for important intellectual content: AH, PW, OA, AL, GS, SC, JH, JS, SIT, EH, AB, JH. Statistical analysis: JH. Obtaining funding: EH. Administrative, technical or material support: GS, PW, EH. Supervision: PW.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflict of interest.
Ethical approval
The regional ethics committee in Gothenburg approved the study 2007/277-07 2007-10-19).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hagman, A., Lantz, A., Carlsson, S. et al. Urinary continence recovery and oncological outcomes after surgery for prostate cancer analysed by risk category: results from the LAParoscopic prostatectomy robot and open trial. World J Urol 39, 3239–3249 (2021). https://doi.org/10.1007/s00345-021-03662-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-021-03662-0