
Abstract
Objective
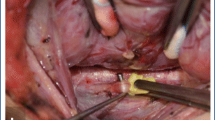
Localization of the vagus nerve is required during intraoperative neuromonitoring (IONM) for thyroid surgery in order to electromyographically verify the functional integrity of inferior laryngeal nerve and aim to reduce the risk of postoperative vocal fold paralysis. Classically, the vagus nerve courses within the carotid sheath between the common carotid artery and internal jugular vein, but anatomic variations have been described. Our aim was to compare preoperative ultrasound (US) and intraoperative localization of vagus nerve and to document anatomic variations.
Patients and methods
Retrospective study of patients undergoing thyroidectomy. The vagus nerve was identified 2 cm below the inferior border of the cricoid cartilage, on US performed 6 weeks prior to surgery; then, vagus nerve was identified surgically.
Results
For 82 patients, on preoperative US, the right vagus nerve was in between, superficial, or deep to the vessels in 94%, 2.4%, and 3.6%, and on the left in 72%, 24.4%, and 3.6%. Intraoperatively, the right vagus was in between, superficial, or deep in 90%, 4%, and 6%, and on the left in 67%, 27%, and 6%. US correlated with surgery on the right in 79/82 (96%) and on the left in 78/82 (95%).
Conclusions
To our knowledge, this is the first study directly comparing US and intraoperative findings. The US and surgical findings were identical in 95% on the left and 96% on the right The vagus nerve was superficial in 27% of cases on the left and 4% on the right. Identifying this anatomic variation preoperatively may facilitate IONM.
Key Points
• Localization of the vagus nerve is necessary during thyroid surgery when using neuromonitoring for electromyographic testing of the inferior laryngeal nerve to reduce the risk of postoperative vocal fold paralysis.
• The vagus nerve in the neck can be routinely visualized using ultrasound, and is generally in between the common carotid artery and the internal jugular vein. Its location on ultrasound corresponds very closely to that observed in vivo during surgery (95%).
• At the level of the thyroid lobe, there is an anatomic variant with the vagus nerve superficial to the common carotid artery which is seen more often on the left than on the right.





Similar content being viewed by others


Abbreviations
- CC:
-
Common carotid artery
- IJ:
-
Internal jugular vein
- IONM:
-
Intraoperative neuromonitoring
- mA:
-
Milliampere
- SD:
-
Standard deviation
- US:
-
Ultrasound
References
Randolph GW, Dralle H, International Intraoperative Monitoring Study G et al (2011) Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: international standards guideline statement. Laryngoscope 121(Suppl 1):S1–S16
Wu CW, Dionigi G, Chen HC et al (2013) Vagal nerve stimulation without dissecting the carotid sheath during intraoperative neuromonitoring of the recurrent laryngeal nerve in thyroid surgery. Head Neck 35:1443–1447
Phelan E, Schneider R, Lorenz K et al (2014) Continuous vagal IONM prevents recurrent laryngeal nerve paralysis by revealing initial EMG changes of impending neuropraxic injury: a prospective, multicenter study. Laryngoscope 124:1498–1505
Hojaij F, Rebelo G, Akamatsu F et al (2019) Syntopy of vagus nerve in the carotid sheath: a dissectional study of 50 cadavers. Laryngoscope Investig Otolaryngol 4:319–322
Ha EJ, Baek JH, Lee JH, Kim JK, Shong YK (2011) Clinical significance of vagus nerve variation in radiofrequency ablation of thyroid nodules. Eur Radiol 21:2151–2157
Berthoud HR, Neuhuber WL (2000) Functional and chemical anatomy of the afferent vagal system. Auton Neurosci 85:1–17
Yigit E, Dursun E, Omeroglu E et al (2018) The course of lower cranial nerves within the neck: a cadaveric dissection study. Eur Arch Otorhinolaryngol 275:2541–2548
Dionigi G, Chiang FY, Rausei S et al (2010) Surgical anatomy and neurophysiology of the vagus nerve (VN) for standardised intraoperative neuromonitoring (IONM) of the inferior laryngeal nerve (ILN) during thyroidectomy. Langenbecks Arch Surg 395:893–899
Knappertz VA, Tegeler CH, Hardin SJ, McKinney WM (1998) Vagus nerve imaging with ultrasound: anatomic and in vivo validation. Otolaryngol Head Neck Surg 118:82–85
Park JK, Jeong SY, Lee JH, Lim GC, Chang JW (2011) Variations in the course of the cervical vagus nerve on thyroid ultrasonography. AJNR Am J Neuroradiol 32:1178–1181
Kikuta S, Jenkins S, Kusukawa J, Iwanaga J, Loukas M, Tubbs RS (2019) Ansa cervicalis: a comprehensive review of its anatomy, variations, pathology, and surgical applications. Anat Cell Biol 52:221–225
Kikuta S, Iwanaga J, Kusukawa J, Tubbs RS (2019) An unusual superior root of the ansa cervicalis. Cureus 11:e4558
Jelev L (2013) Some unusual types of formation of the ansa cervicalis in humans and proposal of a new morphological classification. Clin Anat 26:961–965
Banneheka S, Tokita K, Kumaki K (2008) Nerve fiber analysis of ansa cervicalis-vagus communications. Anat Sci Int 83:145–151
Abu-Hijleh MF (2005) Bilateral absence of ansa cervicalis replaced by vagocervical plexus: case report and literature review. Ann Anat 187:121–125
Miyake N, Hayashi S, Kawase T et al (2010) Fetal anatomy of the human carotid sheath and structures in and around it. Anat Rec (Hoboken) 293:438–445
Funding
The authors state that this work has not received any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Dr. Dana Hartl.
Conflict of interest
The authors of this manuscript declare relationships with the following companies: Dr. Hartl has received consulting fees from Medtronic®.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Ethical approval
Institutional Review Board approval was obtained.
Study subjects or cohorts overlap
None of the study subjects or cohorts has been previously reported.
This study was presented as an e-poster at the Francophone Congress of Radiology (“Journées Francophones de Radiologie”), Paris, France, October 11–14, 2019.
Methodology
• retrospective
• observational
• performed in only one center
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hartl, D.M., Bidault, S., Girard, E. et al. Ultrasound visualization of the vagus nerve for intraoperative neuromonitoring in thyroid surgery. Eur Radiol 31, 4063–4070 (2021). https://doi.org/10.1007/s00330-020-07472-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-020-07472-7