
Abstract
Objectives
To retrospectively review the radiological and clinicopathological features of gliosarcoma (GSM) and differentiate it from glioblastoma multiforme (GBM).
Methods
The clinicopathological data and imaging findings (including VASARI analysis) of 48 surgically and pathologically confirmed GSM patients (group 1) were reviewed in detail, and were compared with that of other glioblastoma (GBM) cases in our hospital (group 2).
Results
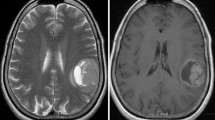
There were 28 men and 20 women GSM patients with a median age of 52.5 years (range, 24-80 years) in this study. Haemorrhage (n = 21), a salt-and-pepper sign on T2-weighted images (n = 36), unevenly thickened wall (n = 36) even appearing as a paliform pattern (n = 32), an intra-tumoural large feeding artery (n = 32) and an eccentric cystic portion (ECP) (n = 19) were more commonly observed in the GSM group than in GBM patients. Based on our experience, GSM can be divided into four subtypes according to magnetic resonance imaging (MRI) features. When compared to GBM (group 2), there were more patients designated with type III lesions (having very unevenly thickened walls) and IV (solid) lesions among the GSM cases (group 1). On univariate prognostic analysis, adjuvant therapy (radiotherapy, chemotherapy, and radiochemotherapy) and existence of an eccentric cyst region were prognostic factors. However, Cox's regression model showed only adjuvant therapy as a prognostic factor for GSM.
Conclusions
When compared to GBM, certain imaging features are more likely to occur in GSM, which may help raise the possibility of this disease. All GSM patients are recommended to receive adjuvant therapy to achieve a better prognosis with radiotherapy, chemotherapy or radiochemotherapy all as options.
Key Points
• Diagnosis of gliosarcoma can be suggested preoperatively by imaging.
• Gliosarcoma can be divided into four subtypes based on MRI.
• Paliform pattern and ECP tend to present in gliosarcoma more than GBM.
• The cystic subtype of gliosarcoma may predict a more dismal prognosis.
• All gliosarcoma patients should receive adjuvant therapy to achieve better prognosis.






Similar content being viewed by others


Abbreviations
- ECP:
-
Eccentric cystic portion
- GBM:
-
Glioblastoma multiforme
- GSM:
-
Gliosarcoma
- HGG:
-
High-grade glioma
- IHC:
-
Immunohistochemical
- OS:
-
Overall survival
- PSM:
-
Propensity score matching
- VASARI:
-
Visually accessible rembrandt images
References
Buckner JC, Ballman KV, Michalak JC et al (2006) Phase III trial of carmustine and cisplatin compared with carmustine alone and standard radiation therapy or accelerated radiation therapy in patients with glioblastoma multiforme: North Central Cancer Treatment Group 93-72-52 and Southwest Oncology Group 9503 Trials. J Clin Oncol 24:3871–3879
Kozak KR, Mahadevan A, Moody JS (2009) Adult gliosarcoma: epidemiology, natural history, and factors associated with outcome. Neuro Oncol 11:183–191
Han SJ, Yang I, Tihan T, Prados MD, Parsa AT (2010) Primary gliosarcoma: key clinical and pathologic distinctions from glioblastoma with implications as a unique oncologic entity. J Neurooncol 96:313–320
Walker GV, Gilbert MR, Prabhu SS, Brown PD, McAleer MF (2013) Temozolomide use in adult patients with gliosarcoma: an evolving clinical practice. J Neurooncol 112:83–89
Frandsen J, Orton A, Jensen R et al (2017) Patterns of care and outcomes in gliosarcoma: an analysis of the National Cancer Database. J Neurosurg 21:1–6
Sampaio L, Linhares P, Fonseca J (2017) Detailed magnetic resonance imaging features of a case series of primary gliosarcoma. Neuroradiol J 30:546–553
Louis DN, Perry A, Reifenberger G et al (2016) The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol 131:803–820
Damodaran O, van Heerden J, Nowak AK et al (2014) Clinical management and survival outcomes of gliosarcomas in the era of multimodality therapy. J Clin Neurosci 21:478–481
Stupp R, Hegi ME, Mason WP et al (2009) Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol 10:459–466
Stupp R, Mason WP, van den Bent MJ et al (2005) Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352:987–996
Cao H, Wang F, Li XJ (2017) Future strategies on glioma research: from big data to the clinic. Genomics Proteomics Bioinformatics 15:263–265
Liao W, Liu Y, Wang X et al (2009) Differentiation of primary central nervous system lymphoma and high-grade glioma with dynamic susceptibility contrast-enhanced perfusion magnetic resonance imaging. Acta Radiol 50:217–225
Chang K, Bai HX, Zhou H et al (2017) Residual convolutional neural network for determination of IDH status in low- and high-grade gliomas from MR imaging. Clin Cancer Res 2018, 24(5):1073-1081.
Zhou H, Vallières M, Bai HX et al (2017) MRI features predict survival and molecular markers in diffuse lower-grade gliomas. Neuro-Oncology 19:862–870
Wanggou S, Feng C, Xie Y, Ye L, Wang F, Li X (2016) Sample level enrichment analysis of KEGG pathways identifies clinically relevant subtypes of glioblastoma. J Cancer 7:1701–1710
Singh G, Das KK, Sharma P et al (2015) Cerebral gliosarcoma: analysis of 16 patients and review of literature. Asian J Neurosurg 10:195–202
Maiuri F, Stella L, Benvenuti D, Giamundo A, Pettinato G (1990) Cerebral gliosarcomas: correlation of computed tomographic findings, surgical aspect, pathological features, and prognosis. Neurosurgery 26:261–267
di Norcia V, Piccirilli M, Giangaspero F, Salvati M (2008) Gliosarcomas in the elderly: analysis of 7 cases and clinico-pathological remarks. Tumori 94:493–496
Han L, Zhang X, Qiu S et al (2008) Magnetic resonance imaging of primary cerebral gliosarcoma: a report of 15 cases. Acta Radiol 49:1058–1067
Meis JM, Martz KL, Nelson JS (1991) Mixed glioblastoma multiforme and sarcoma. A clinicopathologic study of 26 radiation therapy oncology group cases. Cancer 67:2342–2349
Zhang BY, Chen H, Geng DY et al (2011) Computed tomography and magnetic resonance features of gliosarcoma: a study of 54 cases. J Comput Assist Tomogr 35:667–673
NCBI/NCI/The Cancer Imaging Archive (TCIA) (2016), VASARI (Visually AcceSAble Rembrandt Images) MRI feature set, NCBI/NCI, Bethesda MD. Available via https://wikicancerimagingarchivenet/display/Public/VASARI+Research+Project. Accessed 25 July 2016
Machuca TN, Prevedello DM, Pope LZ, Haratz SS, Araújo JC, Torres LF (2004) Gliosarcoma: report of four cases with immunohistochemical findings. Arq Neuropsiquiatr 62:608–612
Lutterbach J, Guttenberger R, Pagenstecher A (2001) Gliosarcoma: a clinical study. Radiother Oncol 61:57–64
Acknowledgements
Dr. Xiaoping Yi is right now a Postdoctoral Fellow in Postdoctoral Research Workstation of Pathology and Pathophysiology, Basic Medical Sciences, Xiangya Hospital, Central South University (No. 185705). We thank all the members of Department of Radiology and Professor Li’s Lab, Xiangya Hospital, for helpful discussion.
Funding
This study has received funding by the National Natural Science Foundation of China (No. 81472594, 81770781)
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Professor Xuejun Li.
Conflict of interest
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Ethical approval
Institutional Review Board approval was obtained.
Methodology
• retrospective
• case-control study
• performed at one institution
Rights and permissions
About this article

Cite this article
Yi, X., Cao, H., Tang, H. et al. Gliosarcoma: a clinical and radiological analysis of 48 cases. Eur Radiol 29, 429–438 (2019). https://doi.org/10.1007/s00330-018-5398-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-018-5398-y