
Abstract
Objectives
Thyroid nodular disease is one of the most commonly observed medical conditions. Cytological evaluation of the specimens obtained with fine-needle aspiration biopsy (FNAB) is the most accurate tool for selecting nodules which should be further surgically removed. A major limitation of this method is the high occurrence of non-diagnostic results. This indicates the need for improvement of the thyroid biopsy technique. The aim of this meta-analysis was to compare the diagnostic value of thyroid core-needle biopsies (CNBs) and FNABs.
Materials and methods
PubMed/MEDLINE, Cochrane Library, Scopus, Cinahl, Academic Search Complete, Web of Knowledge, PubMed Central, PubMed Central Canada and Clinical Key databases were searched. Risk ratios (RRs) of non-diagnostic results were meta-analysed using the random-effects model.
Results
Eleven studies were included in the quantitative analysis. CNB yielded significantly more diagnostic results – the pooled risk ratio (RR) of gaining a non-diagnostic result was 0.27 (p<0.0001). For lesions with one previous non-diagnostic FNAB, RR was 0.22 (p<0.0001).
Conclusions
CNB seems to be a valuable diagnostic technique yielding a higher proportion of diagnostic results than conventional FNAB. It is also significantly more effective in case of nodules with a prior non-diagnostic result of FNAB results than repeated FNABs.
Key Points
• Core-needle biopsy yields a higher proportion of diagnostic results than fine-needle biopsy.
• Core-needle biopsies may decrease the amount of unnecessary thyroidectomies.
• Probability of gaining non-diagnostic result using core-needle biopsy is almost four times lower.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Thyroid nodular disease (TND) is one of the most commonly observed medical conditions, affecting a large number of individuals, especially women, subpopulations in iodine-deficient regions, elderly people and patients with some specific clinical conditions. The prevalence of TND is high, affecting 10–70 % of the general population and malignancies are observed in 3–10 % of patients [1–5]. Cytological evaluation of the specimens obtained with fine-needle aspiration biopsy (FNAB) is the most accurate tool for selecting nodules which should be further surgically removed (malignancies, indeterminate follicular lesions) [6]. One of the major limitations of this method is a high occurrence of non-diagnostic results, falling in group I of the Bethesda Classification [7]. According to numerous studies, around 10–20 % of FNABs yield non-diagnostic results [8–10]. Most endocrinological societies recommend consideration of total thyroidectomy in cases of repeated FNABs with non-diagnostic results [11]. This may increase the number of unnecessary thyroidectomies and also delay the final diagnosis of thyroid cancer. This indicates the need for improvement of the thyroid biopsy technique or even searching for new tools which may decrease the prevalence of non-diagnostic results. Biopsy with the use of a core needle (CNB) is believed to be reliable improvement on FNAB, bringing high diagnostic yield [12, 13]. The aim of the current meta-analysis was to compare the diagnostic value of thyroid CNBs and FNABs.
Materials and methods
Study selection
PubMed/MEDLINE, Cochrane Library, Scopus, Cinahl, Academic Search Complete, Web of Knowledge, PubMed Central, PubMed Central Canada and Clinical Key databases from January 2001 up to December 2014 were searched in order to find all relevant, full-text journal articles written in English. We used the search term: ((“core-needle”) or (core and needle)) and thyroid. Articles comparing the percentage of diagnostic results of thyroid FNAB and CNB, performed with sonographic guidance, were included in the meta-analysis. According to the Bethesda System for Reporting Thyroid Cytopathology [14], categories II–VI are interpreted as diagnostic results. Samples classified as Bethesda category III and IV are inconclusive results in the context of differentiation between benign and malignant lesions but assessed as adequate for cytological assessment. We excluded studies about very particular groups of lesions (e.g. hyalinasing trabecular tumours, follicular tumours) and studies where FNAB or CNB was performed without ultrasound guidance. Studies without control groups, comparing results of FNAB with FNAB and CNAB performed simultaneously (without distinct data about the FNAB and CNAB results) were systematically reviewed.
Two researchers (K.W. and A.S.) searched all included databases independently and prepared a list of included studies. In case of discrepancies between lists, authors read questionable articles together.
Quality assessment of the studies
All included studies were assessed using the Newcastle-Ottawa Scale [15]. Studies with a result of seven stars or more were included.
Statistical analysis
All calculations were performed using Statistica v.10 with the medical package from Statsoft. Risk ratios (RRs) of non-diagnostic result were meta-analysed using the random-effects model. Publication bias was assessed using Kendall’s tau.
Results
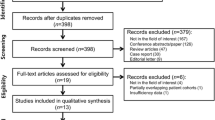
The search results and steps of selection are shown in the flowchart (Fig. 1). Eleven studies were included to the meta-analysis – the basic data are shown in Table 1 [6, 16–25]. CNB yielded significantly a higher amount of diagnostic results. The forest plot is shown on Fig. 2. The pooled RR of non-diagnostic results was 0.27 with a 95 % confidence interval (CI) 0.16–0.46 (p<0.0001). There is no evidence for publication bias (Kendall’s tau = −0.24, two-tailed p-value = 0.31). There was evidence of significant heterogeneity (Q =85.3, df=10, i2=88.3 %, p<0.0001).

Flowchart showing the steps included in the literature search and selection
(Table 2)

Forest plot showing individual and pooled risk ratios (RRs) of gaining non-diagnostic results with core-needle biopsy in comparison to fine-needle aspiration biopsy; with 95 % confidence intervals and p-values given in columns 2–4
We have also performed some analyses in subgroups.
Seven studies focused on lesions with one previous non-diagnostic result of FNAB [17–21, 23, 24]. The forest plot is shown on Fig. 3. The pooledRR of gaining a non-diagnostic result was 0.22 (95 % CI 0.10–0.45, p=0.0001). There is no evidence for publication bias (Kendall’s tau = −0.33, two-tailed p-value = 0.29). There was evidence of significant heterogeneity (Q =47.5, df=6, i2=87.37 %, p<0.0001).

Cumulative forest plot for studies comparing risk ratios (RRs) of gaining non-diagnostic results with core-needle biopsy in comparison to fine-needle aspiration biopsy; with 95 % confidence intervals and p-values given in columns 2–4
Four studies from South Korea were performed with very similar methodology [17, 18, 20, 23]. Lesions with one previous non-diagnostic FNAB were included, in all studies the ACECUT system by TSK, Japan was used. For these studies the pooled RR was 0.05 (95 % CI 0.02–0.10, p<0.0001). ). There is no evidence for publication bias (Kendall’s tau = 0.0, two-tailed p-value = 1.0). There was no evidence of significant heterogeneity (Q =1.2, df=3, i2=0.0 %, p=0.76).
Discussion
CNB yielded a significantly higher percentage of diagnostic results than FNAB in lesions with previous non-diagnostic results with FNAB. RR was 0.27, which means that the probability of gaining a non-diagnostic result was almost four times lower. However, the number of studies comparing the diagnostic efficacy of FNAB was rather low. We found 11 case-control studies on the topic. In addition, these studies differed with regard to the diameters of needles and design of the study (CNB as the first-line procedure or as a procedure performed after one or more non-diagnostic FNABs, prospective/retrospective character, simultaneous CNB and FNAB, or CNB and FNAB performed in distinct groups of subjects). Among these studies, nine had shown significantly higher diagnostic effectiveness of CNB, in one the difference was not significant [19], and in one FNAB had a significantly higher percentage of diagnostic results with borderline significance [25].
We also performed subgroup analyses. We found seven studies comparing FNAB and CNB in lesions with previous non-diagnostic results with FNAB; however, those studies were diverse in terms of methodology. Among those seven studies, four showed that CNB yielded incomparably higher diagnostic effectiveness – RR of non-diagnostic result <0.1 [17, 18, 20, 23]. According to two studies, CNB was significantly more effective; however, the result was less impressive than that of the four studies mentioned above [21, 24]. Another study did not reveal any advantage of CNB over repeated FNAB [19].
These discrepancies suggest that further studies are strongly recommended. One of the possible reasons could be different diameters of fine and core needles used in particular studies. Stangierski et al. [19] used 25 G fine and 22 G core needles, Samir et al. [21] used 25 and 20 G, respectively; in the study performed by Na et al. [20] 18 G needles were used for CNB and different types of needles for FNAB (21–25 G, proportion unknown), Lee et al. [18] used 18 G core needles, data about fine needles were not given. Similarly, Yeon et al. [26] reported very a high percentage of diagnostic results with CNB with 18 G needles in lesions after one non-diagnostic FNAB (over 98 %); however, this study was not included in the meta-analysis due to the lack of a control group.
Another possible reason for this heterogeneity could result from many variables, rather difficult to meta-analyse, such as experience of the radiologist/endocrinologist performing the biopsy, number of passes, equipment used, etc. Four studies performed using similar equipment (automatic biopsy guns from the same manufacturer) in patients with one previous non-diagnostic FNAB showed very homogenous results [17, 18, 20, 23]. This fact can suggest that equipment used and group of patients selected are the most important factors influencing the findings; homogeneity in these two areas resulted in very homogenous results. Pooled results of these studies were very impressive – the risk of gaining a non-diagnostic result was 20 times lower than in the case of FNAB. According to this data, automatic biopsy guns can be helpful in patients with non-diagnostic results with FNAB. However, the invasiveness of the procedure should also be taken into account.
Another aspect worth considering is a pain sensation among patients undergoing both kinds of procedures. The number of studies on this topic is limited. Reports performed by Stangierski et al. [19] and Nasrollah et al. [27] indicate CNB is slightly more painful than FNAB; however, it is tolerable for most patients. But it is worth keeping in mind that the difference in the diameter of core and fine needles in both studies was quite small – 21G versus 23G. In a study performed by Capri et al. [28], fine needles and large needles were used. The authors report no difference in pain sensation accompanying the two procedures; however, a small amount of anaesthesia was injected subcutaneously before the biopsy. According to the accessible data, it seems that the use of core needles is not accompanied by patient intolerance and a severe pain sensation.
The current study constitutes a large meta-analysis which aims to systematize this important topic. An interesting study on this issue was published by Trimboli et al. in 2014 [29]. These authors found and briefly described many previously published studies. However, it was systematic review so there was no quantitative synthesis of the results. There was also one conceptually similar meta-analysis published by Li et al. [30]. However, the authors of that study included a smaller number of studies, five, whereas 11 studies were included in the current study. Partially this difference can be explained by the fact that quite a few studies have been published recently and were not available for Li et al. [16–19]. A greater number of included studies allowed for additional analyses in subgroups (e.g. comparison of FNAB and CNB in lesions with one previous non-diagnostic FNAB). Finally, the meta-analysis published by Li et al. brought some confounding results: a visible, but nonsignificant difference in the diagnostic values of FNAB and CNB. Our study including more studies provides more definite, clinically important conclusions.
In conclusion, the CNB seems to be a valuable diagnostic technique yielding a higher proportion of diagnostic results than conventional FNAB. It is also significantly more effective in cases of nodules with prior non-diagnostic results with FNAB than repeated FNABs. However, further studies on the topic are required.
References
Tan GH, Gharib H (1997) Thyroid incidentalomas: management approaches to nonpalpable nodules discovered incidentally on thyroid imaging. Ann Intern Med 126:226–231
Szczepanek-Parulska E, Woliński K, Stangierski A et al (2013) Comparison of diagnostic value of conventional ultrasonography and shear wave elastography in the prediction of thyroid lesions malignancy. PLoS ONE 8(11), e81532
Wolinski K, Czarnywojtek A, Ruchala M (2014) Risk of Thyroid Nodular Disease and Thyroid Cancer in Patients with Acromegaly – Meta-Analysis and Systematic Review. PLoS ONE 9(2), e88787
Stanicić J, Prpić M, Jukić T, Borić M, Kusić Z (2009) Thyroid nodularity - true epidemic or improved diagnostics. Acta Clin Croat 48:413–418
Ruchała M, Szczepanek-Parulska E, Fularz M, Woliński K (2012) Risk of neoplasms in acromegaly. Contemp Onco (Pozn) 16:111–117
Renshaw AA, Pinnar N (2007) Comparison of thyroid fine-needle aspiration and core needle biopsy. Am J Clin Pathol 128:370–374
Raab SS, Vrbin CM, Grzybicki DM et al (2006) Errors in thyroid gland fine needle aspiration. Am J Clin Pathol 125:873–882
Baier ND, Hahn PF, Gervais DA et al (2009) Fine-needle aspiration biopsy of thyroid nodules: experience in a cohort of 944 patients. AJR Am J Roentgenol 193:1175–1179
Zhong LC, Lu F, Ma F et al (2015) Ultrasound-guided fine-needle aspiration of thyroid nodules: does the size limit its efficiency? Int J Clin Exp Pathol 8:3155–3159
Seningen JL, Nassar A, Henry MR (2012) Correlation of thyroid nodule fine-needle aspiration cytology with corresponding histology at Mayo Clinic, 2001-2007: an institutional experience of 1,945 cases. Diagn Cytopathol 40(Suppl 1):E27–32
Haugen BR, Alexander EK, Bible KC et al (2016) 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 26:1–133
Paja M, Del Cura JL, Zabala R et al (2016) Ultrasound-guided core-needle biopsy in thyroid nodules. A study of 676 consecutive cases with surgical correlation. Eur Radiol 26:1–8
Ha EJ, Baek JH, Lee JH, et al. Core needle biopsy could reduce diagnostic surgery in patients with anaplastic thyroid cancer or thyroid lymphoma. Eur Radiol. 2015 Jul 23. [Epub ahead of print]
Cibas ES, Ali SZ; NCI Thyroid FNA State of the Science Conference (2009) The Bethesda System For Reporting Thyroid Cytopathology. Am J Clin Pathol 132:658–665
Wells GA, Shea B, O’Connell D, et al (2000) The Newcastle-Ottawa scale (nos) for assessing the quality of nonrandomized studies in meta-analyses. The 3rd symposium on systematic reviews: Beyond the basics. Oxford, England
Chen BT, Jain AB, Dagis A et al (2014) Comparison of Efficacy and Safety of Ultrasound-Guided Core Needle Biopsy versus Fine Needle Aspiration for Evaluating Thyroid Nodules. Endocr Pract. doi:10.4158/EP14303.OR
Choi SH, Baek JH, Lee JH et al (2014) Thyroid nodules with initially non-diagnostic, fine-needle aspiration results: comparison of core-needle biopsy and repeated fine-needle aspiration. Eur Radiol 24:2819–2826
Lee SH, Kim MH, Bae JS et al (2014) Clinical outcomes in patients with non-diagnostic thyroid fine needle aspiration cytology: usefulness of the thyroid core needle biopsy. Ann Surg Oncol 21:1870–1877
Stangierski A, Wolinski K, Martin K, Leitgeber O, Ruchala M (2013) Core needle biopsy of thyroid nodules - evaluation of diagnostic utility and pain experience. Neuro Endocrinol Lett 34:798–801
Na DG, Kim JH, Sung JY et al (2012) Core-needle biopsy is more useful than repeat fine-needle aspiration in thyroid nodules read as nondiagnostic or atypia of undetermined significance by the Bethesda system for reporting thyroid cytopathology. Thyroid 22:468–475
Samir AE, Vij A, Seale MK et al (2012) Ultrasound-guided percutaneous thyroid nodule core biopsy: clinical utility in patients with prior nondiagnostic fine-needle aspirate. Thyroid 22:461–467
Sung JY, Na DG, Kim KS et al (2012) Diagnostic accuracy of fine-needle aspiration versus core-needle biopsy for the diagnosis of thyroid malignancy in a clinical cohort. Eur Radiol 22:1564–1572
Park KT, Ahn SH, Mo JH et al (2011) Role of core needle biopsy and ultrasonographic finding in management of indeterminate thyroid nodules. Head Neck 33:160–165
Strauss EB, Iovino A, Upender S (2008) Simultaneous fine-needle aspiration and core biopsy of thyroid nodules and other superficial head and neck masses using sonographic guidance. AJR Am J Roentgenol 190:1697–1699
Karstrup S, Balslev E, Juul N, Eskildsen PC, Baumbach L (2001) US-guided fine needle aspiration versus coarse needle biopsy of thyroid nodules. Eur J Ultrasound 13:1–5
Yeon JS, Baek JH, Lim HK et al (2013) Thyroid nodules with initially nondiagnostic cytologic results: the role of core-needle biopsy. Radiology 268:274–280
Nasrollah N, Trimboli P, Rossi F et al (2013) Patient’s comfort with and tolerability of thyroid core needle biopsy. Endocrine 45:79–83
Carpi A, Rossi G, Nicolini A et al (2013) Does large needle aspiration biopsy add pain to the thyroid nodule evaluation? PLoS ONE 8(3), e58016
Trimboli P, Crescenzi A (2015) Thyroid core needle biopsy: taking stock of the situation. Endocrine 48:779–785
Li L, Chen BD, Zhu HF et al (2014) Comparison of pre-operation diagnosis of thyroid cancer with fine needle aspiration and core-needle biopsy: a meta-analysis. Asian Pac J Cancer Prev 15:7187–7193
Khoo TK, Baker CH, Hallanger-Johnson J et al (2008) Comparison of ultrasound-guided fine-needle aspiration biopsy with core-needle biopsy in the evaluation of thyroid nodules. Endocr Pract 14:426–431
Zhang S, Ivanovic M, Nemcek AA Jr et al (2008) Thin core needle biopsy crush preparations in conjunction with fine-needle aspiration for the evaluation of thyroid nodules: a complementary approach. Cancer 114:512–518
Mehrotra P, Hubbard JG, Johnson SJ et al (2005) Ultrasound scan-guided core sampling for diagnosis versus freehand FNAC of the thyroid gland. Surgeon 3:1–5
Harvey JN, Parker D, De P, Shrimali RK, Otter M (2005) Sonographically guided core biopsy in the assessment of thyroid nodules. J Clin Ultrasound 33:57–62
Screaton NJ, Berman LH, Grant JW (2003) US-guided core-needle biopsy of the thyroid gland. Radiology 226:827–832
Acknowledgments
The scientific guarantor of this publication is Prof. Marek Ruchala, Head of the Department of Endocrinology, Metabolism and Internal Medicine, Poznan University of Medical Sciences. The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. This study was supported by the Poznan University of Medical Sciences, Faculty of Medicine II (grant nr 502-14-02221354-41127). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
One of the authors has significant statistical expertise. Institutional Review Board approval was not required because the study is a meta-analysis. Written informed consent was waived by the Institutional Review Board. Some study subjects or cohorts have not been previously reported.
Methodology: meta-analysis, performed at one institution.
Author information
Authors and Affiliations
Corresponding author
Additional information
Kosma Wolinski and Adam Stangierski contributed equally to this work.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Wolinski, K., Stangierski, A. & Ruchala, M. Comparison of diagnostic yield of core-needle and fine-needle aspiration biopsies of thyroid lesions: Systematic review and meta-analysis. Eur Radiol 27, 431–436 (2017). https://doi.org/10.1007/s00330-016-4356-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-016-4356-9