
Abstract
The use of online surveys as a recruitment tool for clinical research has recently expanded; nevertheless, optimal recruitment strategies remain poorly identified. Objectives. The study aimed to identify the most effective recruitment strategies for online research studies and to determine the optimal survey channels for obtaining patients’ responses. This is a post-hoc analysis of the ARCOVAX (ArLAR COVID Vaccination) study. Multiple recruitment strategies were disseminated in Arabic, English, and French. The proportion of enrolled patients was correlated with each strategy. Channels used by patients to complete the survey were divided into three categories (social media (SoMe), doctor, and patients’ associations). These channels were correlated with the patients’ characteristics and the country’s Gross Domestic Product (GDP). A total of 1595 patients from 19 Arab countries completed the survey. Patients’ mean age was 39 years, 73.2% (1159) were females, 17.8% (284) had a university education level and 93.1% (1468) answered the survey in Arabic. The most effective recruitment strategies were personalized WhatsApp reminders to recruiters (30% of enrolled patients), technical support in response to access issues (27%) and sharing recruitment status by country on a WhatsApp group (24%). The channels used to complete the survey were: SoMe in 45% (711), doctor in 40% (647), and patients’ associations in 8.5% (233), and correlated with age and GDP. To optimize recruitment, it is recommended to combine multiple strategies and channels, use the native language and be active (mobilize teams), reactive (provide prompt technical support), and proactive (share regular updates and reminders).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Online surveys are currently one of the most effective tools for recruiting participants for clinical research [1] and have been largely stimulated by the Coronavirus Disease 2019 (COVID-19) pandemic. Using e-recruitment, a web-based recruitment method and a mass communication medium, researchers are now able to reach a large patient population [2]. Analysis of the most effective strategies to promote recruitment for online research studies is crucial to ensure that the right approach is used in the right population to properly meet its needs.
One of the major channels to disseminate online surveys is social media (SoMe), such as Facebook, Twitter, or WhatsApp. In fact, SoMe has been widely used for specific health-related purposes, especially after the COVID-19 outbreak, such as medical education, awareness campaigns, health interventions, and medical surveillance [3]. Its use for recruiting participants in health surveys is growing and shows many advantages compared to traditional methods [4, 5]. It stimulates interest in participants, increases engagement and retention of subjects, and provides better interaction between clinical research demand and supply [6, 7]. Moreover, it improves participation, especially in hard-to-reach populations [8], reduces the cost, offers flexibility in time and place, and accelerates the rate of recruitment [4]. In particular, WhatsApp, which is the most used mobile instant messaging, optimizes immediate communication between the researcher and the participant at an affordable price, offering flexibility in time and place [9].
However, e-recruitment might have a negative impact on the quality of data collection, on the diversity of participants, and is more prone to technical issues [10]. Indeed, online surveys create more selection bias and inadequacy of population representation since samples obtained tend to be younger, more educated, and with a female predominance [8]. Also, electricity and internet access in certain populations remain a barrier to recruitment through SoMe [4]. Other issues, such as the validity of informed consent and protection of privacy are also of concern [6].
Literature about online recruitment for research studies lacks detailed information about the profile of participants, optimal recruitment strategies and survey channels, especially in Arab countries.
The ARCOVAX study (Arab League of Associations for Rheumatology (ArLAR) Vaccination study) [11] is a cross-sectional study that used an anonymous web-based survey to assess the acceptability of the COVID-19 vaccine in patients with chronic rheumatic musculoskeletal diseases (RMDs) and healthcare professionals (HCPs) and included participants from 16 Arab countries. Being one of the largest recent online surveys in the region, the ARCOVAX population represents an excellent opportunity to analyze the optimal e-recruitment strategies.
The primary objective of this study was to identify the most effective recruitment strategies for online research studies, based on the ARCOVAX study. The secondary objective was to determine the optimal survey channels for collecting the patients’ responses.
Methods
Study design
This is a post hoc analysis of the ARCOVAX study adapted from the VAXICOV study [12, 13], translated to Arabic by a steering committee composed of ten rheumatologists and one rheumatology fellow. The survey was validated by the ArLAR scientific committee composed of rheumatologists from 16 Arab countries. The scientific committee made a few minor revisions, with regard to the different names of medications in the different countries. A pilot test done in three languages (Arabic, English, and French) found the survey to be well understood and easy to complete in less than 10 min. The survey was disseminated online in the three languages between April 13 and May 11, 2021. Health-care professionals were considered as a convenience control group, expected to serve as a reference for optimal vaccine acceptability at the time of the study. The study included 1595 patients and 1517 HCPs by convenience sampling. Nevertheless, the two groups were very different in terms of socio-demographic characteristics, therefore, the current study was focused on the patient group.
Main outcome variable
The survey channels used by the participants to respond were recorded and grouped into three categories: SoMe platforms in general, the doctor (by direct contact at the clinic or through WhatsApp messaging), and patients’ associations.
Procedures
At launch, the survey was disseminated online using the Google Forms platform, through multiple SoMe platforms (Facebook, Twitter, Instagram, Snapchat, Messenger, WhatsApp groups) of ArLAR, Arab Adult Arthritis Awareness group (AAAA, an ArLAR special-interest group), a network of participating rheumatologists within ArLAR and patient associations’ accounts. In addition, mass emails were sent from the ArLAR and the AAAA group to available mailing lists of HCPs and patients with RMDs. Also, WhatsApp messages were shared on the participating rheumatologists’ groups to be sent to their available patients’ WhatsApp lists. Finally, posters with QR codes were created and displayed in the participating rheumatology clinics. During the recruitment period, additional strategies were used to boost e-recruitment: weekly reminders on SoMe and WhatsApp groups, sharing regular recruitment status by country on AAAA WhatsApp group which included the key recruiters, personalized WhatsApp messages sent to key recruiters, providing real-time technical support in case of survey access issues (such as technical assistance in connection with the survey link in the preferred languages), announcing the count-down to the last days of recruitment using a motivational video on SoMe.
Anonymous demographic data were collected: age, gender, educational level, rheumatic disease, anti-rheumatic treatments, vaccine perceptions, country, and Gross Domestic Product (GDP) level according to the World Bank Classification [14]. The details of the questionnaire were previously described elsewhere [11].
Ethical considerations
Accessing the Google Form platform and then clicking “Agree” after reading the survey description was considered as consent to participate. Confidentiality was maintained in the study by keeping all the participants’ data anonymous. The study was approved by the scientific committee of the ArLAR and by the Institutional Review Boards of Saint-Joseph University, Beirut, and the Specialized Medical Center, Riyadh (respectively, numbers CEHDF1825 and H-01-R-056, both in April 2021).
Statistical analysis
The participants’ profiles (demographic and disease characteristics and chronic anti-rheumatic treatments) were presented descriptively as numbers and percentages for categorical variables and means and standard deviations for continuous variables.
The characteristics related to the survey were recorded: language used to respond to the survey, number of responses according to the country, and the GDP region [13].
For this study, we identified 5 sequential strategies to boost e-recruitment: (1) Launching the survey on a Social Media platform, (2) providing real-time technical support in case of survey access issues such as technical assistance in connection with the survey link in the preferred languages, (3) sharing regular recruitment status by country on AAAA WhatsApp group which included the key recruiters, (4) displaying reminder posters with QR codes in the participating rheumatology clinics, (5) personalized WhatsApp messages sent to key recruiters, (6) announcing the count-down to the last days of recruitment using a motivational video on SoMe.
Each strategy used to boost e-recruitment was presented descriptively in correlation with the number of daily enrolments over the time period of recruitment (from April 13 to May 11, 2021) and with the proportion of participants enrolled immediately after the instauration of the strategy.
Also, three channels used to reach the patients were identified: (1) Public messages via any SoMea platform including Facebook, Instagram, Twitter, Snapchat, Messenger, WhatsApp groups (2) Patients’ associations on SoMe and (3) one on one contact with the doctor (either by direct contact at the clinic or through WhatsApp message from the doctors’ office). The factors associated with each channel were identified using Chi-Square, Fisher exact test, and ANOVA as appropriate. A p value < 0.05 was used to define statistical significance. All statistical analyses were performed on JAMOVI 2021 version 1.6 [15].
Results
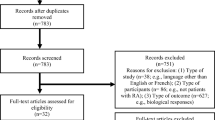
A total of 3176 participants from 19 Arab countries completed the survey, from which 1595 patients with RMDs were included in the current analysis.
Profile of the participants
The mean age of the patients was 39 years (SD 13 years); 72.7% were females and 17.8% had a university education (Table 1). The patients were from High-Income countries in 36.2%, Upper-Middle Income countries in 34.1%, and Low-Middle and Low-Income countries in 29.6%.
Language used in the survey
The majority of patients responded to the survey in Arabic (93.1%) followed by French (4.3%) and English (2.6%). However, significant differences among the countries were found. For instance, more responses in French were received from the Maghreb countries (Algeria, Morocco, and Tunisia countries) and Lebanon (p < 0.001) (Fig. 1).

Enrollment of patients for the online survey and correlation with the recruitment strategies. WA WhatsApp Messages, *sharing the status with key recruiters
Day of the week
The higher rate of response to the survey was observed on Mondays (21.9%), followed by Wednesdays (18.5%) and Tuesdays (15.2%), which are weekdays in all the surveyed countries.
The rate of participation
The recruitment of participants was highly fluctuating throughout the study period (Fig. 2). The first peak of inclusion was observed on day 3, after providing prompt technical support for participants having access issues, and a second peak was observed on day 14, after sending a personalized reminder to key recruiters. About 50% of the participants were enrolled in the first 10 days of the recruitment period which lasted around one month in total. In addition, more than 90% of the participants were enrolled within the first 21 days, after which there seemed to be a saturation effect.

Language chosen by patients to respond to the ARCOVAX survey, by country and geographical region
Online recruitment strategies had a different impact on the rate of participation: 30% of participants were enrolled after sending personalized WhatsApp reminders to key recruiters in different countries, 27% after providing prompt technical support to resolve issues faced by the participants, 24% after sharing recruitment status by country on the AAAA's WhatsApp group, 12% after posting electronic posters and QR codes via SoMe and WhatsApp groups, 3% after the initial launch on SoMe and WhatsApp groups and 2% after sharing a motivational video announcing the countdown to the last week of recruiting.
Survey channels for collecting patients’ responses
Among the 1595 patients, 711 (44.7%) patients were recruited via anonymous SoMe (Facebook, Instagram, Twitter, Snapchat), 647 (40.7%) were recruited through their doctor (either by direct contact at the clinic or through WhatsApp message from the doctors’ office), and only 233 (14.6%) were recruited through patients’ associations. Less than 1% (15 patients) were recruited through emails.
Factors associated with patient participation through social media
The use of SoMe channel to participate in the survey was highest in Lower-Middle and Low-Income countries (53.6% of participants from these countries were reached through SoMe), followed by High-Income countries (48.9%) and Upper-Middle-Income countries (32.2%) (p < 0.001).
Patients who used SoMe to participate were younger (mean age 38.2 years [SD 11.6]) compared to those who used other channels (39.7 years [SD 14.1]). No association was found with gender (p = 0.10), language (p = 0.64) and education (p = 0.66) (Table 2).
Factors associated with patient participation through the doctor
The survey reached the patients through their doctors mainly in the Upper Middle-Income countries (56.6% of the patients from that GDP region). This channel was also associated with older age (mean age was 40.3 years [SD 14.8] in patients who were reached through their doctor versus 38.2 years [SD 11.6] in the other channels (p = 0.002) (Table 2).
Factors associated with patient participation through the patients’ associations
The proportion of patients who were reached through the patients’ association was small in general (8.5%) but was slightly higher in the High-Income countries (9.1%) (p < 0.001) (Table 2).
Discussion
The most effective e-recruitment strategies for patients with RMDs for research purposes were personalized WhatsApp reminders to the key recruiters, especially in Middle-Income countries, and prompt technical support, mostly in high-income countries. The superiority of personalized messages over mass-produced messages and random posts on SoMe was reported in previous studies [16], highlighting the importance of empathy among researchers and participants. Indeed, participants’ compliance increases with their familiarity with the one making the request. In addition, the remarkable boost in response rate seen after the correction of technical issues suggests the importance of this action in all online surveys as mentioned in the literature [17].
Moreover, this study clearly demonstrated that an Arabic version of an international survey is mandatory to reach the participants living in Arab countries. However, French was also important in the Maghreb countries and Lebanon, where it is the second language. Thus, the current study confirmed that the native language is always the best way to reach a population since it offers a comprehensive form of a survey that gives less biased results and is more practical for the patient to finish the survey faster [18].
Regarding the optimal survey channels for reaching the patients, the current study highlights the importance of SoMe, especially in the younger population. This fact is concordant with previous literature [19, 20] which demonstrated that SoMe has become a global phenomenon and plays a central role in increasing participation levels. The importance of SoMe was observed in all countries regardless of the GDP levels but was more pronounced in Low to Low-Middle Income countries (53.6% of participants). Nevertheless, doctors still play a significant role as well to improve recruitment. The “doctor’s” channel should not be underestimated especially in Upper Middle-income countries where 56.6% of patients were recruited through their doctors. Finally, an important point highlighted by our data was the urgent need to activate the role of patients’ associations since only 8.5% of patients were recruited through this channel, mostly in high-income countries.
The profile of participants was consistent with the literature that showed that younger patients [21, 22] and females [34] were more likely to respond to online surveys. In comparison with the VAXICOV study [12] Arab patients who responded to the ARCOVAX survey were younger, with a mean age of 39 ± 13 years, compared to a mean age of 50 ± 10 years in VAXICOV. Also, 72.7% of participants were identified as females in the ARCOVAX study, whereas 90.5% of participants in the VAXICOV study were females. With Information Technology (IT) development, the young participants are much more reachable through SoMe [23]. Moreover, the young population tends to be more involved in health education and more motivated to participate in medical surveys, whereas older patients may not realize the importance of contributing to medical studies. As for gender, the female predominance may reflect the higher female/male ratio in some RMDs such as rheumatoid arthritis or lupus [24]. Moreover, females could be more responsive to online surveys because they tend to be more patient, interested in health education, and available since in Arab countries, many females do not work [25].
This study has some limitations. First, a selection bias should be considered, as SoMe was used to promote the survey, which would undoubtedly impact the profile of participants. Moreover, the data about individual platforms (i.e., Facebook or Twitter alone) was not available for analysis; thus, profiling patients by platform type was not possible. Although the use of SoMe might be very heterogeneous among the Arab countries, it has a very strong and growing presence, with a predominance of Facebook use [26]. In a previous ArLAR survey including 2163 patients with RMDs, 73% reported that their main source of information about COVID-19 was obtained through SoMe, followed by television in 51% [27]. Nevertheless, a large number of participants (3176 participants, including 1595 patients) can give a reasonably accurate idea about the target population of patients with RMDs. In addition, and since the socio-demographic profiles of patients and HCPs were very different, only the patients were included in the current analysis, to minimize the risk of confounding bias in the analysis of factors associated with the use of the communication channel. Also, one might argue that there’s an overlap between the channels for reaching the patient. For example, a patient might be reached by their doctors through the latter’s SoMe account or by WhatsApp. However, we estimate that the patients identified in priority the channel they considered as the primary channel for receiving the survey. Moreover, although the association between one strategy and the subsequent recruitment was clear in the descriptive analysis, one might argue that the recruitment may also be boosted by previous strategies having a residual effect over time. Finally, the study did not consider the severity of the disease. In fact, a relationship could exist between disease severity and the motivation to respond to a survey related to the disease, as studies showed that knowledge of the topic increases the participation rate [28]. Despite these limitations, the study followed the current directives for survey-based studies, i.e., having an ethical committee approval, survey validation by a different group than the authors, pilot testing, maintaining anonymity, using various social media platforms, and utilization of descriptive and analytical approaches, which adds to the data quality and conformity with international guidance [1, 29, 30].
In summary, the most effective strategies to promote recruitment for online research studies were sending personalized reminders to key recruiters, followed by providing prompt technical support, and sharing enrollment results by country in real-time. Moreover, the importance of SoMe, as well as the role of doctors as a recruitment channel were highlighted crucial. Disparities and variations according to GDP classification and age were noted. Furthermore, the study confirmed the participation of a predominantly young and female patient profile, and higher participation in the native Arabic language. Therefore, to optimize recruitment, it is recommended to combine multiple strategies and channels, use the native language, and be active (mobilize teams to participate), reactive (provide prompt technical support), and proactive (share regular updates and reminders).
Data availability
Data can be made available upon request from the corresponding author.
References
Ball HL (2019) Conducting online surveys. J Hum Lact 35(3):413–417. https://doi.org/10.1177/0890334419848734
Smith AD, Manna DR (2005) E-recruitment of patients for clinical trials. Int J Electron Healthc 1(4):413. https://doi.org/10.1504/IJEH.2005.006688
Chen J, Wang Y (2021) Social media use for health purposes: systematic review. J Med Internet Res 23(5):1–16. https://doi.org/10.2196/17917
Whitaker C, Stevelink S, Fear N (2017) The Use of facebook in recruiting participants for health research purposes: a systematic review. J Med Internet Res 19(8):e290. https://doi.org/10.2196/jmir.7071
Rolls K, Hansen M, Jackson D, Elliott D (2016) How health care professionals use social media to create virtual communities: an integrative review. J Med Internet Res 18(6):e166. https://doi.org/10.2196/jmir.5312
Refolo P, Sacchini D, Minacori R, Daloiso V, Spagnolo AG (2015) E-recruitment based clinical research: notes for research ethics committees/institutional review boards. Eur Rev Med Pharmacol Sci 19(5):800–804 (PMID: 25807433)
Frandsen M, Thow M, Ferguson SG (2016) The effectiveness of social media (Facebook) compared with more traditional advertising methods for recruiting eligible participants to health research studies: a randomized controlled clinical trial. JMIR Res Protoc 5(3):e161. https://doi.org/10.2196/resprot.5747
Topolovec-Vranic J, Natarajan K (2016) The use of social media in recruitment for medical research studies: a scoping review. J Med Internet Res 18(11):e286. https://doi.org/10.2196/jmir.5698
Kaufmann K, Peil C (2020) The mobile instant messaging interview (MIMI): using WhatsApp to enhance self-reporting and explore media usage in situ. Mobile Media Com 8(2):229–246. https://doi.org/10.1177/2050157919852392
Barber L (2006) e-Recruitment developments. Inst Employ Stud. https://doi.org/10.2196/resprot.5747
El Kibbi L, Metawee M, Hmamouchi I, Abdulateef N, Halabi H, Eissa M, El Rakawi M, Masri B, Abutiban F, Hamdi W, Adnan A, Najm AA, Felten R, Arnaud L, Ziadé N (2022) Acceptability of the COVID-19 vaccine among patients with chronic rheumatic diseases and health-care professionals: a cross-sectional study in 19 Arab countries. Lancet Rheumatol Mar 4(3):160–163. https://doi.org/10.1016/S2665-9913(21)00368-4
Felten R, Dubois M, Ugarte-Gil MF et al (2021) Vaccination against COVID-19: Expectations and concerns of patients with autoimmune and rheumatic diseases. Lancet Rheumatol 3(4):e243–e245. https://doi.org/10.1016/S2665-9913(21)00039-4
Felten R, Dubois M, Ugarte-Gil MF et al (2021) Cluster analysis reveals three main patterns of beliefs and intention with respect to SARS-CoV-2 vaccination in patients with autoimmune and inflammatory diseases. Rheumatology (Oxford) 60(SI):SI68–SI76. https://doi.org/10.1093/rheumatology/keab432
World Bank Country and Lending Groups–World Bank Data Help Desk (2019). The World Bank. Published online 2019:1–8. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups%0A Accessed 10 April 2022
The jamovi project (2021). jamovi. (Version 1.6) [Computer Software]. Retrieved from https://www.jamovi.org. Accessed 10 April 2022
Yuan P, Bare MG, Johnson MO, Saberi P (2014) Using Online Social Media for Recruitment of Human Immunodeficiency Virus-Positive Participants: A Cross-Sectional Survey. J Med Internet Res 16(5):e117. https://doi.org/10.2196/jmir.3229
Park K, Park N, Heo W, Gustafson K (2018) What prompts college students to participate in online surveys? Int Educ Stud 12(1):69. https://doi.org/10.5539/ies.v12n1p69
Walsh T, Nurkka P, Petrie H, Olsson J (2013) The effect of language in answering qualitative questions in user experience evaluation web-surveys. Proceedings of the 25th Australian Computer-Human Interaction Conference: Augmentation, Application, Innovation, Collaboration, OzCHI 2013. Published online 2013:73–82. https://doi:https://doi.org/10.1145/2541016.2541049
Cobanoglu C, Moreo PJ, Warde B (2001) A comparison of Mail, Fax and Web-based survey methods. Int J Mark Res 43(4):1–15. https://doi.org/10.1177/147078530104300401
Greenlaw C, Brown-Welty S (2009) A comparison of Web-based and paper-based survey methods. Eval Rev 33(5):464–480. https://doi.org/10.1177/0193841x09340214
Aerny-Perreten N, Domínguez-Berjõn MF, Esteban-Vasallo MD, García-Riolobos C (2015) Participation and factors associated with late or non-response to an online survey in primary care. J Eval Clin Pract 21(4):688–693. https://doi.org/10.1111/jep.12367
Listyowardojo TA, Nap RE, Johnson A (2011) Demographic differences between health care workers who did or did not respond to a safety and organizational culture survey. BMC Res Notes 4:328. https://doi.org/10.1186/1756-0500-4-328
Perrin A (2005) Social Media Usage: 2005–2015. (October):2005–2015. www.pewinternet.org/2015/10/08/social-networking-usage-2005-2015/. Accessed 10 April 2022
Ziade N, el Khoury B, Zoghbi M et al (2020) Prevalence and pattern of comorbidities in chronic rheumatic and musculoskeletal diseases: the COMORD study. Sci Rep 10(1):7683. https://doi.org/10.1038/s41598-020-64732-8
El-Swais M (2016) Despite high education levels, Arab women still don’t have jobs. March 9:1–6. https://blogs.worldbank.org/arabvoices/despite-high-education-levels-arab-women-still-don-t-have-jobs. Accessed 10 April 2022
https://gs.statcounter.com/social-media-stats. Accessed 10 April 2022
Ziadé N, El Kibbi L, Hmamouchi I, Abdulateef N et al (2020) Impact of the COVID-19 pandemic on patients with chronic rheumatic diseases: a study in 15 Arab countries. Int J Rheum Dis 23(11):1550–1557. https://doi.org/10.1111/1756-185X.13960
Brosnan K, Kemperman A, Dolnicar S (2021) Maximizing participation from online survey panel members. Int J Mark Res 63(4):416–435. https://doi.org/10.1177/1470785319880704
Gaur PS, Zimba O, Agarwal V, Gupta L (2020) Reporting Survey Based Studies – a Primer for Authors. J Korean Med Sci 35(45):e398. https://doi.org/10.3346/jkms.2020.35.e398
Jones TL, Baxter MA, Khanduja V (2013) A quick guide to survey research. Ann R Coll Surg Engl 95(1):5–7. https://doi.org/10.1308/003588413X13511609956372
Funding
None.
Author information
Authors and Affiliations
Contributions
IH, RF, LA and NZ designed the study. IH, NZ and AAN drafted the first version of the manuscript.IH, AAN, LK, MM, HH, NA, ME, MR, BM, FA, WH, and NZ recruited the participants. All the authors contributed to the critical revision of the manuscript for important intellectual content, All the authors approved the final version to be published. All the authors agreed to be accountable for all aspects of the work. All co-authors take full responsibility for the integrity of all aspects of the work.
Corresponding author
Ethics declarations
Conflict of interest
None.
Ethical approval
The study was approved by the scientific committee of the ArLAR and by the Institutional Review Boards of Saint Joseph University, Beirut, and Specialized Medical Center, Riyadh.
Consent to participate
Accessing the Google form then clicking “Agree” after reading the survey description was considered as consent to participate.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Hmamouchi, I., Abi Najm, A., El Kibbi, L. et al. How to optimize recruitment strategies of patients with rheumatic and musculoskeletal diseases for online surveys: experience from an international study. Rheumatol Int 43, 705–712 (2023). https://doi.org/10.1007/s00296-022-05195-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-022-05195-0